Move in the Tube: Modern Sternotomy Rehabilitation
Explore how modern evidence is reshaping sternal precautions after cardiac surgery. Learn the principles of Keep Your Move in the Tube (KYMITT), current research, and practical physiotherapy advice for post-sternotomy patients.
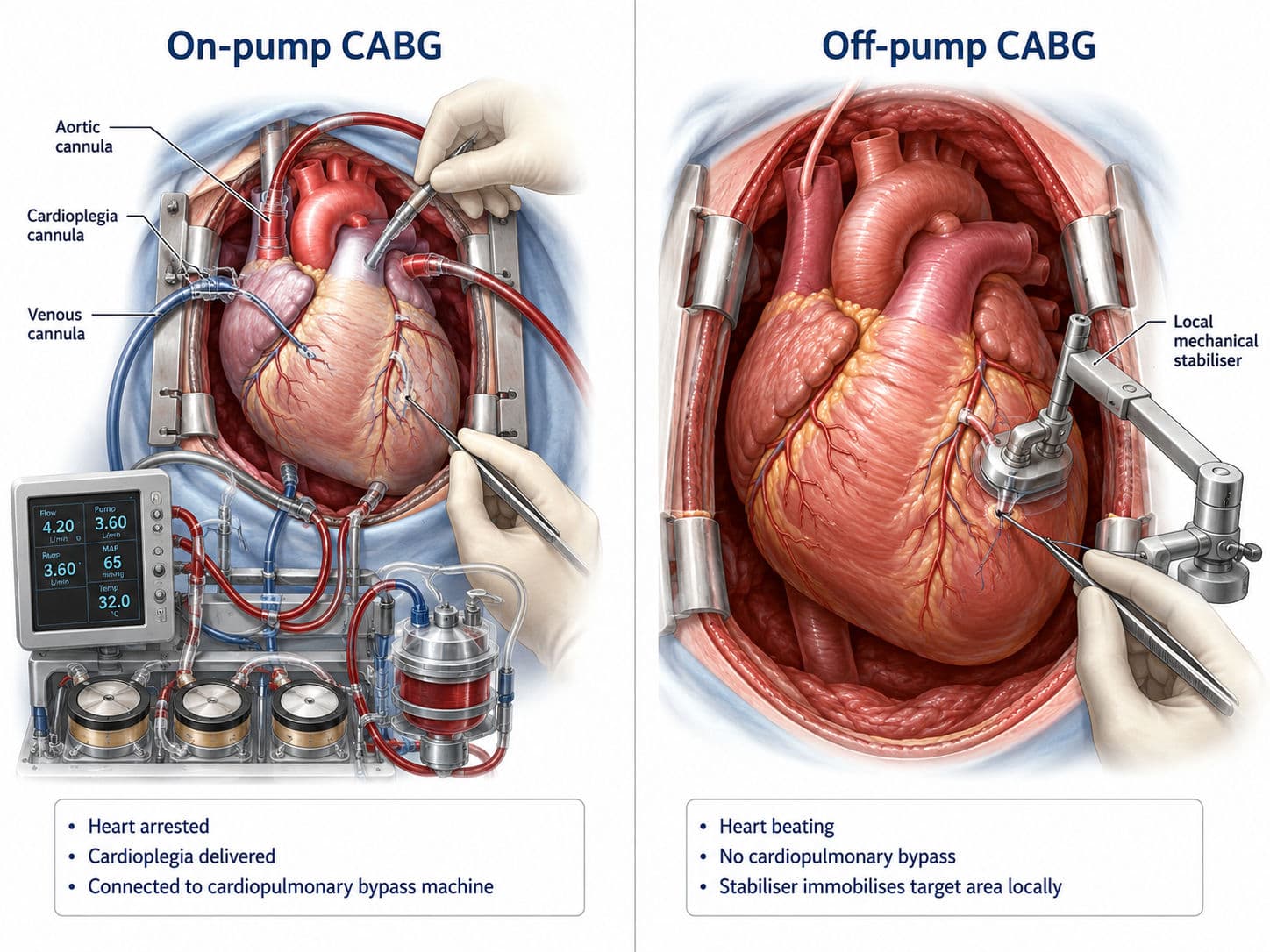
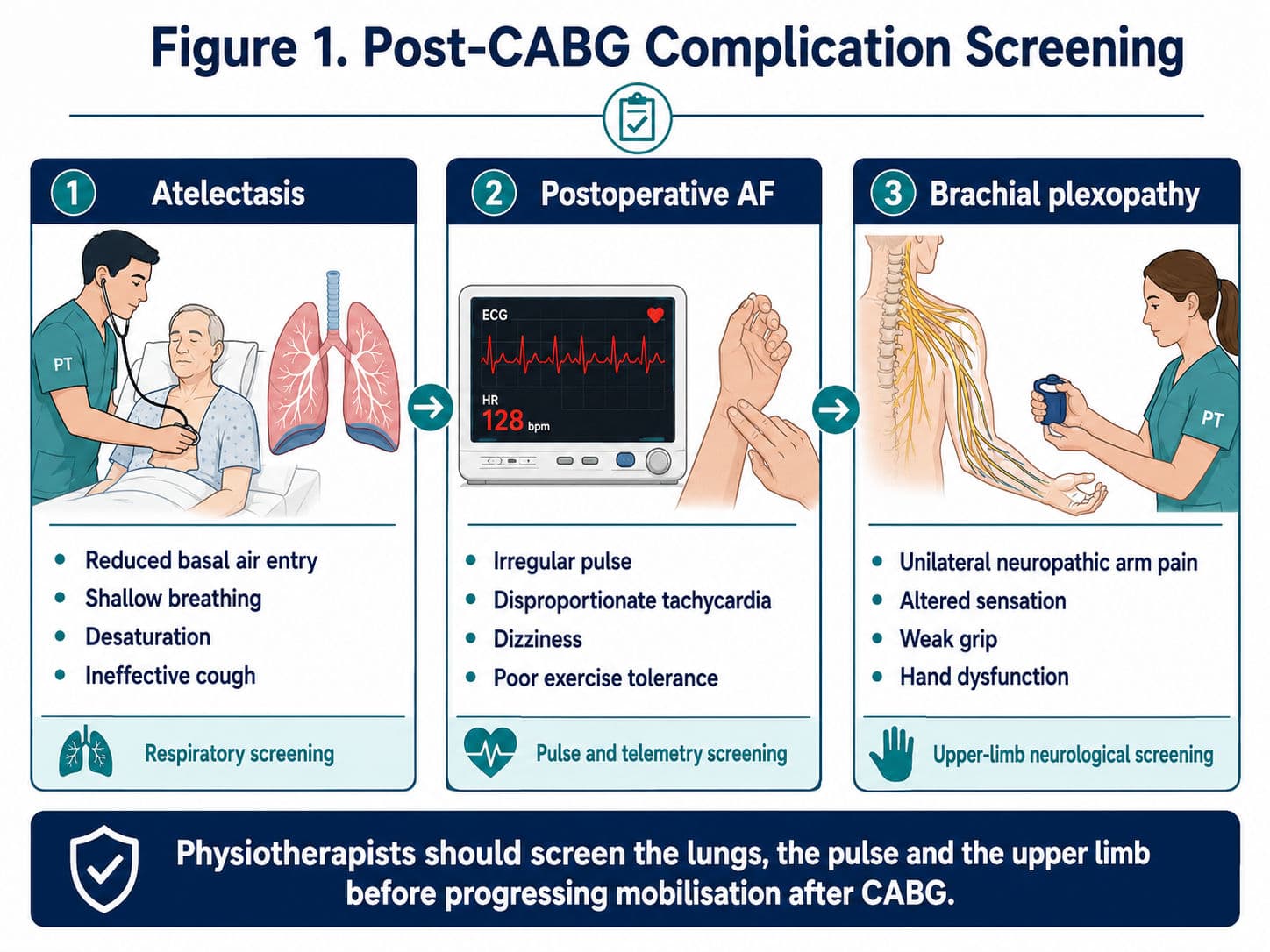
Median sternotomy remains the most common surgical approach for coronary artery bypass grafting (CABG), valve surgery, and many other cardiac procedures. Following surgery, physiotherapists play a critical role in helping patients mobilize safely while protecting the healing sternum. For decades, this balance was achieved through a set of strict activity restrictions known as sternal precautions, which limited lifting, pushing, pulling, and upper-limb use during the early postoperative period.
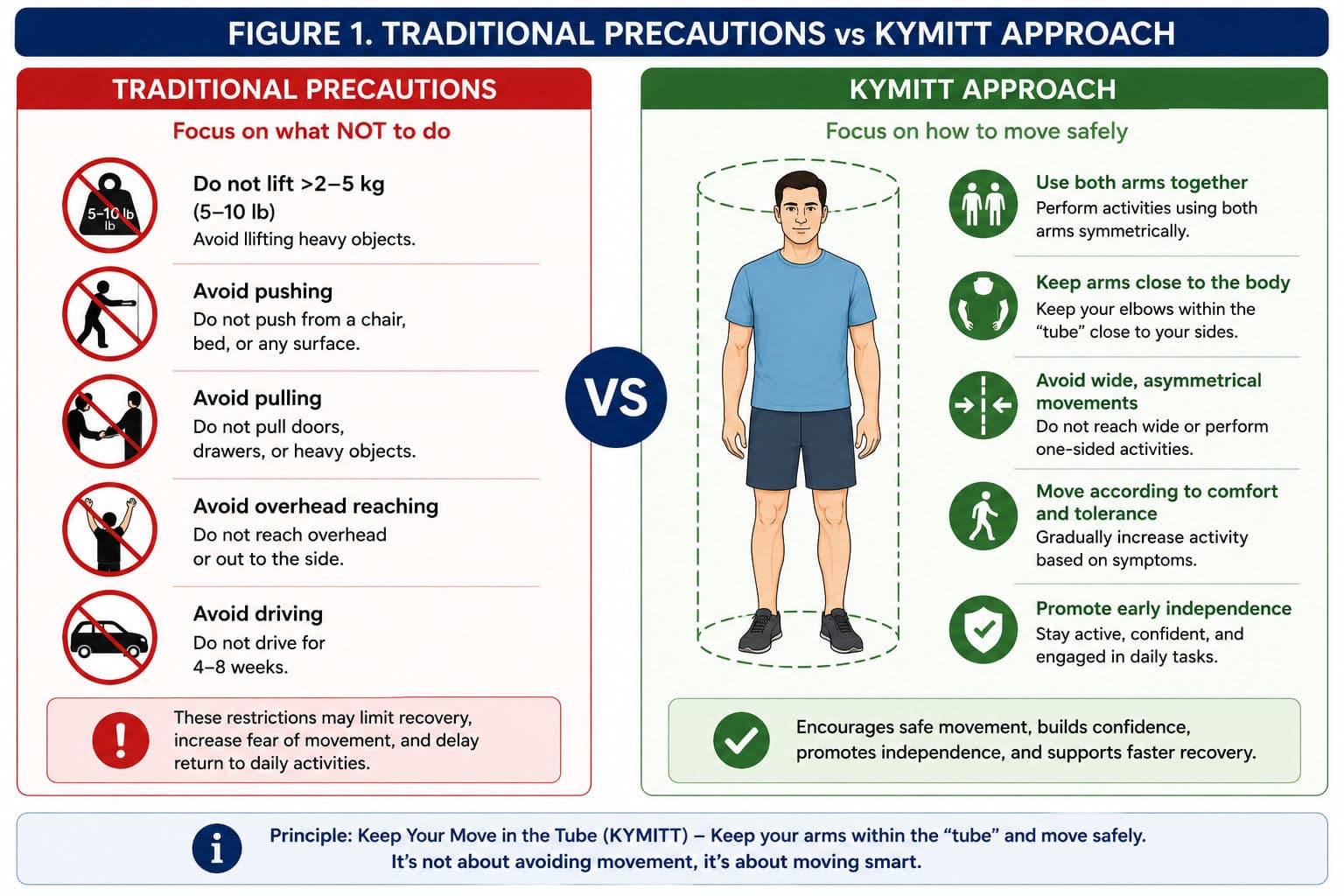
Traditionally, patients were advised not to lift more than 2–5 kg, avoid using their arms to stand from a chair, and refrain from activities such as reaching overhead or driving for several weeks. These precautions became deeply embedded in cardiac rehabilitation programmes worldwide. However, growing research has challenged whether such restrictions are necessary for all patients and whether they may unintentionally delay recovery.
Over the past decade, a more functional and patient-centred approach has emerged. Known as Keep Your Move in the Tube (KYMITT), this concept encourages patients to use their arms during daily activities while maintaining safe movement patterns that minimise excessive stress across the sternum. Understanding this shift from restriction to guided movement is increasingly important for physiotherapy students, clinicians, and exam candidates alike.
Why Did Traditional Sternal Precautions Become Standard Practice?
The rationale behind traditional sternal precautions appears straightforward. During a median sternotomy, the sternum is divided longitudinally and then reapproximated with surgical wires at the end of the procedure. Clinicians historically feared that excessive upper-limb loading could disrupt healing, increase sternal motion, and contribute to complications such as sternal dehiscence, instability, or mediastinitis.
As a result, many hospitals adopted conservative activity restrictions aimed at protecting the healing sternum during the first six to twelve weeks after surgery.
| Traditional Precaution | Common Recommendation |
|---|---|
| Lifting | No more than 2–5 kg (5–10 lb) |
| Pushing and pulling | Avoid whenever possible |
| Sit-to-stand transfers | Avoid using the arms |
| Overhead reaching | Restrict or limit |
| Driving | Avoid for 4–8 weeks |
Although these recommendations became widespread, they were largely developed from expert opinion and surgical caution rather than direct biomechanical evidence. Over time, clinicians began questioning whether universal restrictions were appropriate for every patient recovering from sternotomy.
The Problem with Strict Restrictions
While intended to protect the sternum, traditional precautions can create challenges that extend beyond the surgical site. Many patients become fearful of movement, interpreting postoperative advice as a warning that normal daily activities are dangerous. This fear may reduce participation in rehabilitation, delay functional independence, and increase reliance on caregivers.
For example, a patient who is told not to push with their arms may struggle to stand from a chair despite having sufficient strength and stability to do so safely. Similarly, avoiding arm use during bed mobility can make simple tasks unnecessarily difficult and discourage early activity.
Cahalin and colleagues (2011) highlighted another important issue: significant variation exists between institutions regarding the content and duration of sternal precautions. Some centres restrict lifting for six weeks, while others extend restrictions to three months. Such inconsistency suggests that many recommendations are not strongly supported by evidence.
Furthermore, studies examining the biomechanics of sternotomy recovery have demonstrated that everyday activities often produce less stress across the sternum than forceful coughing. If patients are routinely encouraged to cough for airway clearance, the rationale for prohibiting all upper-limb activity becomes less convincing. These observations prompted researchers to reconsider whether movement quality might be more important than arbitrary weight limits.
Keep Your Move in the Tube: A New Perspective
The Keep Your Move in the Tube (KYMITT) concept was developed to provide a more practical and evidence-informed approach to post-sternotomy rehabilitation. Rather than focusing on what patients should not do, KYMITT emphasises how patients can move safely while remaining active and independent.
The principle is based on an imaginary tube surrounding the trunk. Patients are encouraged to keep their arms close to the body during activities, avoiding wide or asymmetrical movements that may increase stress across the sternum. By maintaining the elbows near the torso and using both arms together, loads can be distributed more evenly through the upper body.

This approach allows patients to participate in everyday activities without unnecessary restrictions. A patient standing from a chair, for example, may use both arms to assist the movement as long as the elbows remain close to the body. Similarly, carrying a light object with both hands near the trunk is considered preferable to reaching with one arm away from the body.
The KYMITT philosophy reflects a broader shift in rehabilitation thinking. Instead of preventing movement, clinicians guide patients toward efficient and symmetrical movement patterns that support healing while maintaining function.
Examples of KYMITT in Practice
- Using both arms during sit-to-stand transfers
- Carrying objects close to the body
- Symmetrical reaching activities
- Assisted bed mobility and rolling
- Functional self-care tasks performed within a comfortable range
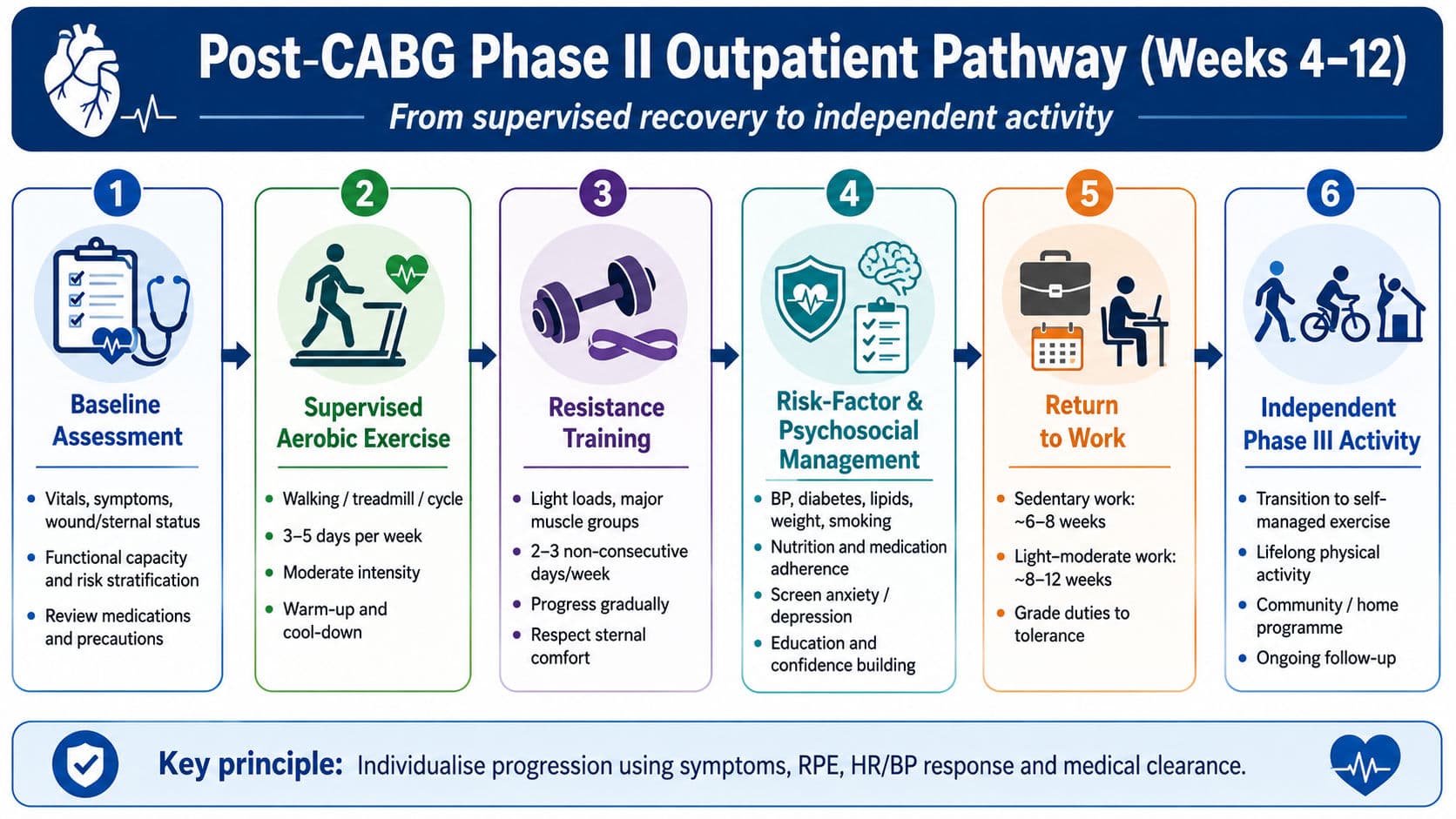
By encouraging confidence and independence, KYMITT aligns closely with contemporary principles of early mobilisation and patient-centred rehabilitation.
What Does the Evidence Say?
The movement toward modern sternal precautions is supported by a growing body of research. One of the earliest and most influential contributions came from Cahalin and colleagues (2011), who reviewed existing precaution practices and questioned the scientific basis for rigid lifting restrictions. The authors argued that many traditional recommendations lacked strong evidence and proposed a more individualised approach to postoperative care.
Adams and colleagues subsequently expanded this concept through biomechanical analysis and clinical observation. Their work emphasised that the manner in which a load is applied may be more important than the absolute amount of weight lifted. Symmetrical movements performed with the arms close to the body appear to create less stress across the sternum than asymmetrical activities, even when the latter involve relatively small loads. These findings formed the foundation of the KYMITT framework and helped shift clinical focus from weight restrictions toward movement quality.
Research by El-Ansary and colleagues further contributed to the understanding of sternal healing. Using imaging techniques to evaluate postoperative sternal motion, they demonstrated that small amounts of movement can occur during normal activities without necessarily indicating pathological instability. Their work reinforced the idea that not all sternal motion is harmful and that patient-specific factors should guide clinical decision-making.
Collectively, the available evidence suggests that most uncomplicated sternotomy patients can safely engage in functional upper-limb activities when appropriate movement strategies are used. Current rehabilitation programmes increasingly favour symptom-guided progression, early mobility, and individualised education rather than universal lifting restrictions.
When Traditional Precautions Still Matter
Despite growing support for the KYMITT approach, traditional precautions have not become obsolete. Certain patients remain at increased risk of impaired sternal healing and may require more conservative management during the postoperative period.
High-risk features include:
- Sternal instability or dehiscence
- Deep sternal wound infection or mediastinitis
- Severe obesity
- Poorly controlled diabetes mellitus
- Osteoporosis
- Chronic corticosteroid use
- Repeat sternotomy procedures
- Prolonged postoperative mechanical ventilation
- Excessive or persistent coughing
In these situations, the potential consequences of sternal complications may outweigh the benefits of early progression. Physiotherapists should therefore assess each patient individually rather than applying a single protocol to all cases.
Regardless of the rehabilitation approach used, clinicians must remain alert for warning signs such as audible clicking, visible sternal movement, wound drainage, increasing pain, or signs of infection. These findings warrant prompt surgical review and may necessitate modification of the rehabilitation programme.
What Would You Advise the Patient?
A common examination question is, "What advice would you give a patient following median sternotomy?”
Encourage the patient to mobilise early and continue normal daily activities using safe movement patterns. Rather than avoiding all arm use, it is advised that one keep the arms close to the body and use both arms symmetrically during activities such as standing, carrying objects, and bed mobility, in accordance with the 'Keep Your Move in the Tube' principle. Activity progression should be guided by symptoms, comfort, wound healing, and overall clinical status. In patients with evidence of sternal instability or risk factors for poor healing, adopt a more conservative approach and monitor closely for complications.

Conclusion
The evolution of sternal precautions reflects a broader transformation within rehabilitation—from rigid restrictions toward guided functional recovery. While traditional precautions were developed with the intention of protecting the healing sternum, modern evidence suggests that many uncomplicated patients benefit from a more active and individualised approach.
The KYMITT concept encourages safe, symmetrical, load-as-tolerated movement while maintaining respect for the biological process of healing. For physiotherapists, the challenge is not simply to protect the sternum but to help patients regain confidence, independence, and functional capacity as early as possible. Understanding when to progress activity and when to remain cautious is central to evidence-based post-sternotomy rehabilitation.
Viva-Ready Summary
- Traditional sternal precautions restricted lifting, pushing, pulling, and arm use after sternotomy.
- Evidence supporting strict weight limits is limited.
- KYMITT encourages patients to use both arms while keeping them close to the body.
- Movement quality is more important than arbitrary lifting thresholds.
- Most uncomplicated sternotomy patients can progress activities according to symptoms and tolerance.
- High-risk sternums may still require temporary traditional precautions.
- Rehabilitation should be individualized rather than protocol driven.
One-Line Recall Point
“Modern sternotomy rehabilitation focuses on safe symmetrical movement, not simply avoiding arm use.”
References
Adams, J., Lotshaw, A., Exum, E., Schmid, K. K., & Dillingham, T. R. (2016). Sternal precautions: Is it time for change? Precautions versus restrictions—a review of literature and recommendations for revision. Cardiopulmonary Physical Therapy Journal, 27(1), 5–15.
Cahalin, L. P., Lapier, T. K., & Shaw, D. K. (2011). Sternal precautions: Time for change. Journal of Cardiopulmonary Rehabilitation and Prevention, 31(1), 8–12.
El-Ansary, D., Waddington, G., Adams, R., & Gibbons, K. (2019). Measurement of non-physiological movement in sternal instability by ultrasound. Physiotherapy Theory and Practice, 35(2), 155–165.
American Association of Cardiovascular and Pulmonary Rehabilitation. (2020). Guidelines for cardiac rehabilitation programs (6th ed.). Human Kinetics.
Frownfelter, D., & Dean, E. (2023). Cardiovascular and pulmonary physical therapy: Evidence to practice (7th ed.). Elsevier.
Hillegass, E. A. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Irwin, S., & Tecklin, J. S. (2024). Cardiopulmonary physical therapy: A guide to practice (7th ed.). Elsevier.