The COPD Spectrum Explained: Chronic Bronchitis, Emphysema, ACO and Bronchiectasis
Learn how to distinguish chronic bronchitis, emphysema, asthma–COPD overlap and bronchiectasis using pathology, clinical features, PFT findings and physiotherapy implications.
A patient with chronic cough, breathlessness and an obstructive pulmonary function test may appear to have straightforward chronic obstructive pulmonary disease (COPD). However, the underlying problem may be mucus-dominant chronic bronchitis, alveolar destruction from emphysema, coexisting asthma and COPD, or structurally damaged bronchi due to bronchiectasis.
These conditions overlap clinically but are not interchangeable. Chronic bronchitis and emphysema are commonly recognised phenotypes within COPD, although both frequently coexist. Asthma–COPD overlap, increasingly described as asthma+COPD, refers to patients with features of both diseases rather than a single universally defined syndrome. Bronchiectasis is a separate structural airway disorder that may mimic or coexist with COPD (Global Initiative for Asthma [GINA], 2025; Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2026).
For physiotherapists, the distinction matters. A mucus-filled airway requires a different treatment priority from a hyperinflated, relatively dry emphysematous lung.
Why Are These Four Conditions Commonly Confused?
All four conditions can present with exertional dyspnoea, cough, wheeze, reduced exercise tolerance and recurrent exacerbations. Spirometry may demonstrate airflow obstruction in each, but the mechanism producing that obstruction differs.
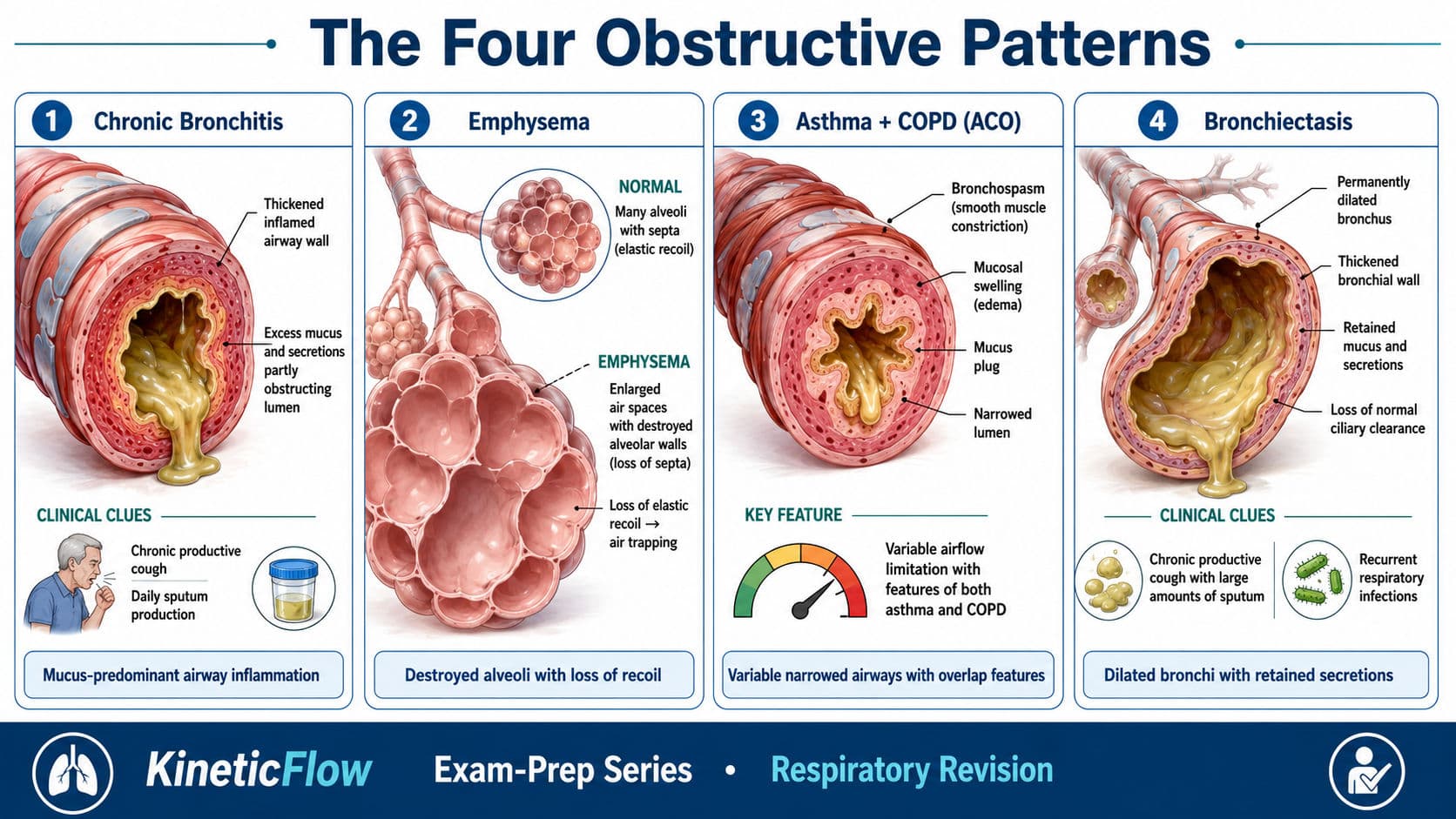
In chronic bronchitis, airflow is limited predominantly by airway inflammation, mucus hypersecretion and narrowing of the smaller bronchi. In emphysema, destruction of alveolar walls and loss of elastic recoil cause expiratory airway collapse and air trapping. In asthma+COPD, persistent COPD-related obstruction occurs alongside features of variable asthma-related airway narrowing. In bronchiectasis, permanently dilated and damaged bronchi promote secretion retention, infection and repeated inflammation.
A useful clinical question is, therefore, the following:
Is the main problem mucus obstruction, loss of elastic recoil, variable bronchospasm or structurally dilated infected airways?
The answer guides both medical management and physiotherapy planning.
The Pathology Behind Each Pattern
Chronic bronchitis: the mucus-predominant pattern
Chronic bronchitis is classically defined as cough with sputum production for at least three months in each of two consecutive years, after excluding alternative causes. Pathologically, irritant exposure produces goblet-cell proliferation, enlargement of mucus-secreting glands, impaired mucociliary clearance and chronic airway inflammation.
Patients usually report a long-standing productive cough, frequent “chest infections” and gradually increasing breathlessness. Coarse crackles, rhonchi or wheezes may be present. However, chronic bronchitis can occur before fixed airflow obstruction develops, so the clinical label alone does not confirm COPD (GOLD, 2026).
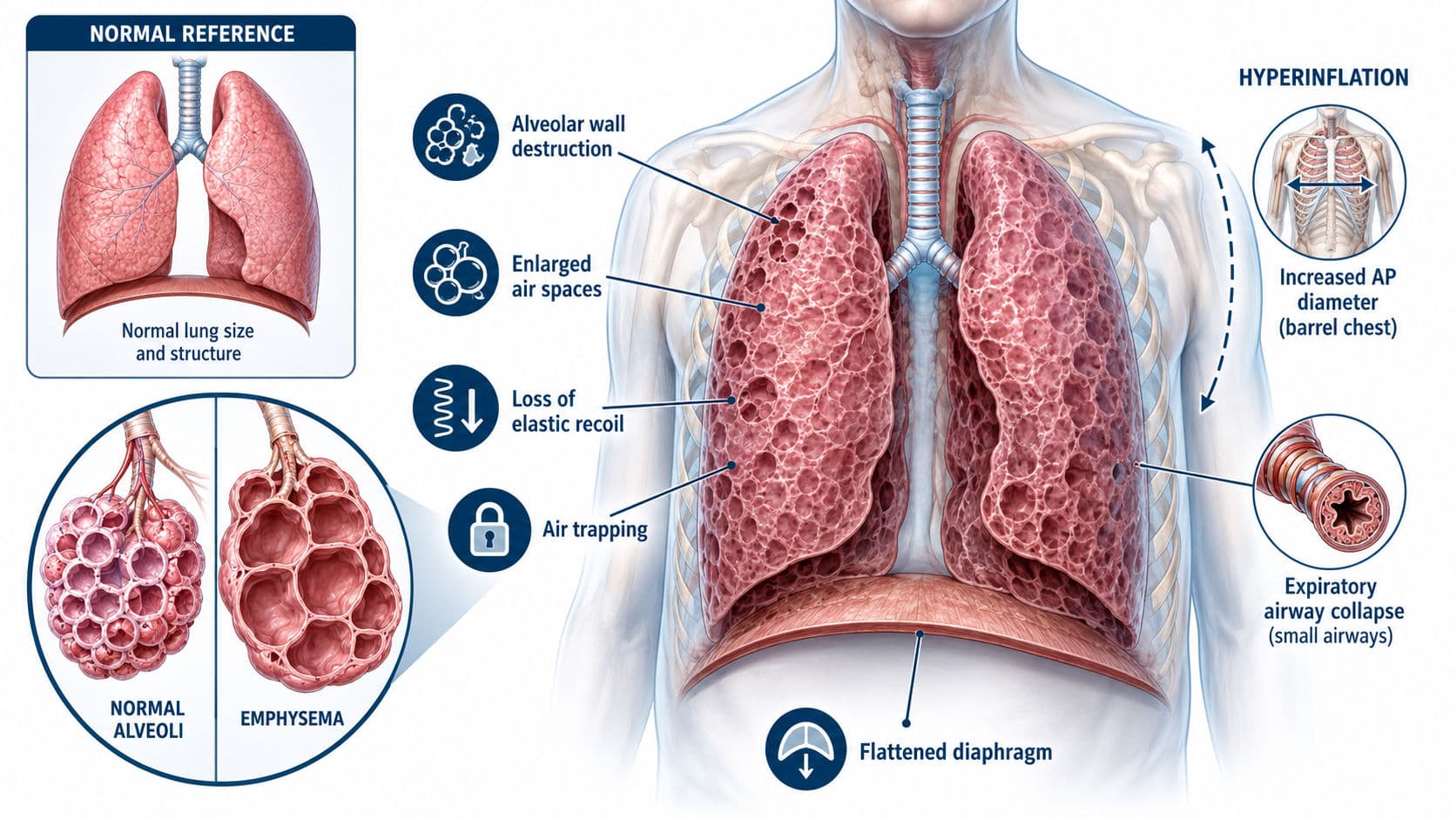
Emphysema: the hyperinflation-predominant pattern
Emphysema is defined pathologically by permanent enlargement of airspaces distal to the terminal bronchioles with destruction of alveolar walls. Loss of alveolar attachments reduces elastic recoil, allowing small airways to collapse during expiration.
The result is air trapping, dynamic hyperinflation, increased work of breathing and reduced gas-exchange surface area. Patients commonly present with progressive exertional dyspnoea, reduced breath sounds, prolonged expiration and use of accessory muscles. Cough may be mild unless chronic bronchitis or another airway disorder is also present.
Asthma+COPD: overlapping clinical features
GINA advises that “asthma+COPD” and “asthma–COPD overlap” should be regarded as descriptive terms rather than one clearly defined disease. Typical clues include a history of asthma, atopy or allergic symptoms; marked variability in symptoms; episodic wheeze; and persistent airflow limitation in an older patient with smoking or occupational exposure.
Because asthma is part of the presentation, pharmacological treatment should include inhaled corticosteroid-containing therapy rather than bronchodilator-only treatment. Physiotherapists should recognise this safety principle while leaving medication prescription and adjustment to the medical team (GINA, 2025).
Bronchiectasis: structurally damaged bronchi
Bronchiectasis involves permanent abnormal dilatation of the bronchi demonstrated on computed tomography, together with compatible clinical symptoms. Impaired clearance permits mucus retention and bacterial infection, creating a cycle of infection, inflammation and further airway damage.
The characteristic presentation is a chronic productive cough with daily sputum, recurrent infective exacerbations and changing sputum volume or purulence. Haemoptysis, coarse inspiratory crackles and fatigue may occur. Unlike uncomplicated chronic bronchitis, bronchiectasis is confirmed structurally on high-resolution computed tomography rather than by symptoms alone (European Respiratory Society [ERS], 2025).
Reading the Pulmonary Function Test Correctly

COPD is confirmed by persistent post-bronchodilator airflow obstruction in the appropriate clinical context. GOLD continues to use a post-bronchodilator FEV₁/FVC below 0.70, whereas ERS/ATS interpretation also emphasises comparison with the lower limit of normal and appropriate reference equations (GOLD, 2026; Stanojevic et al., 2022).
Spirometry alone cannot reliably separate chronic bronchitis from emphysema because both may produce an obstructive pattern. Lung volumes and diffusion capacity provide additional clues:
- High residual volume: this suggests air trapping.
- High total lung capacity: supports hyperinflation, particularly in emphysema.
- Low DLCO (Diffusing Capacity of the Lungs for Carbon Monoxide): supports loss of alveolar-capillary surface area and, therefore, emphysema.
- Relatively preserved DLCO: is more compatible with airway-predominant chronic bronchitis, although mixed disease is common.
A large bronchodilator response may support asthma-related variability but does not independently diagnose asthma+COPD. Conversely, the absence of a large response on one test does not exclude asthma.
In bronchiectasis, pulmonary function may be obstructive, restrictive, mixed or even near normal. The diagnosis therefore depends on the clinical syndrome and CT findings rather than one characteristic spirometric pattern.
One-Page Differentiator Table

Chest X-Ray: Distinguishing the Four Conditions
Chest radiography may provide useful structural clues, but it should not be used alone to diagnose COPD or determine its phenotype. In chronic bronchitis, the chest X-ray may be normal or may show nonspecific prominence of bronchovascular markings, peribronchial thickening and cardiomegaly in advanced disease.
Emphysema produces the most recognisable COPD pattern: hyperlucent and overexpanded lungs, flattened diaphragms, widened intercostal spaces, increased retrosternal airspace and reduced peripheral vascular markings. A long, narrow or vertically oriented cardiac shadow may also be seen.
In asthma+COPD, there is no single diagnostic radiographic pattern; the X-ray may be normal or show temporary hyperinflation when asthma-related bronchospasm predominates, while persistent hyperinflation or vascular attenuation suggests an accompanying emphysematous COPD component.
Bronchiectasis may also be missed on a plain radiograph, particularly in mild disease. More advanced cases may demonstrate thickened bronchial walls, parallel “tram-track” opacities, circular ring shadows, cystic spaces, mucus plugging or focal volume loss. Therefore, high-resolution or thin-section CT remains the confirmatory imaging investigation for bronchiectasis and is more sensitive than chest X-ray for defining emphysema distribution (Global Initiative for Asthma [GINA], 2025; Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2026; Hill et al., 2019).
Radiographic recall:
Chronic bronchitis may look crowded, emphysema looks overexpanded, asthma+COPD shows a variable or mixed pattern, and bronchiectasis may show tram tracks and ring shadows.

How Physiotherapy Priorities Change
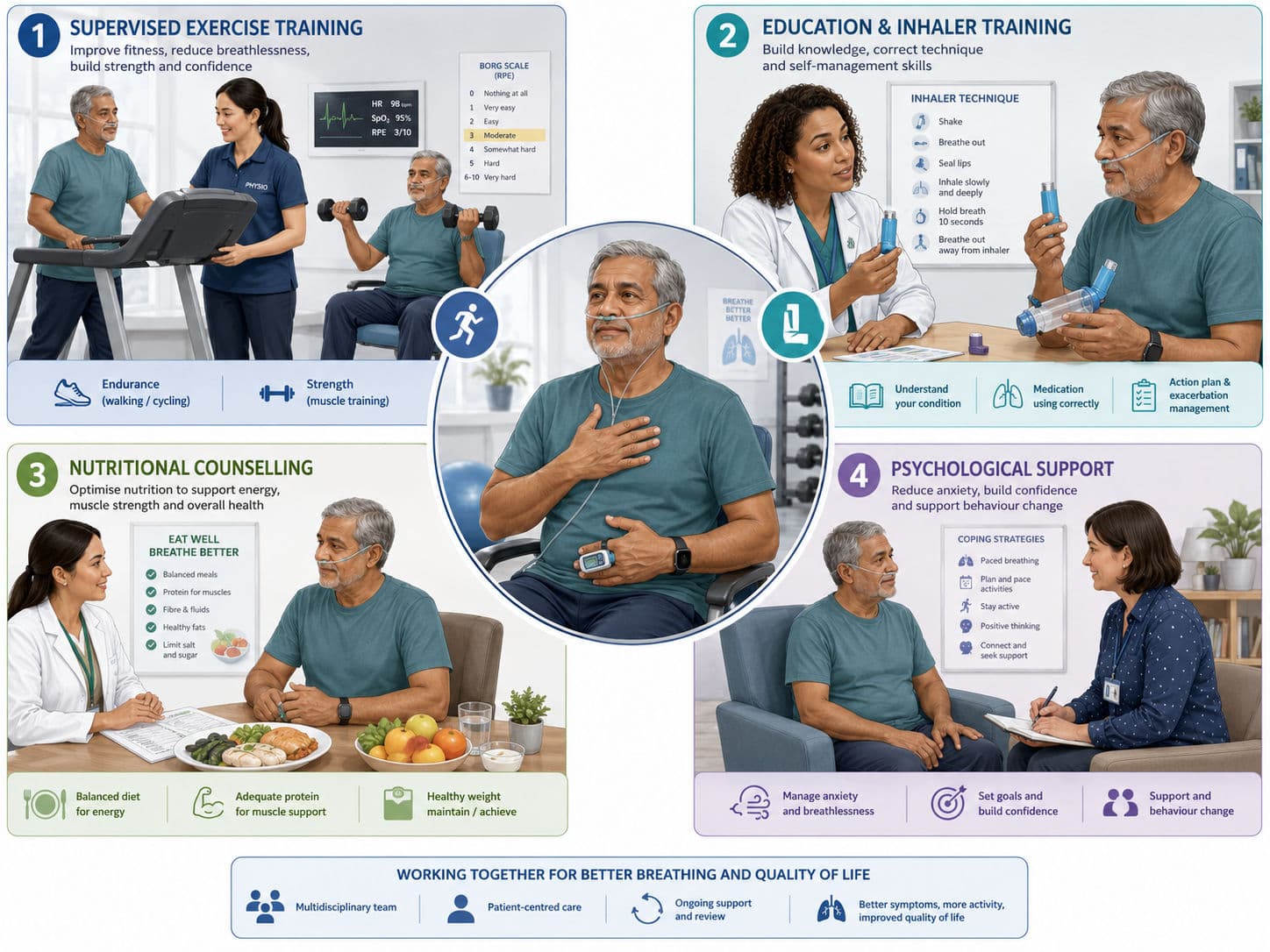
Pulmonary rehabilitation remains a central intervention for symptomatic people with COPD. Exercise training, education, self-management and behavioural support improve dyspnoea, exercise capacity and health-related quality of life (American Thoracic Society, 2023). The programme should be individualised using symptom response, oxygen saturation, functional testing and relevant comorbidities.
In chronic bronchitis, airway clearance is considered when secretion retention is clinically significant. Active cycle of breathing techniques, huffing, positive expiratory pressure or selected positioning may be used after assessing sputum load, airflow limitation, reflux and tolerance. Airway clearance should not be prescribed automatically to every patient labelled as having COPD.
In emphysema, treatment focuses more strongly on reducing ventilatory demand and improving functional efficiency. Pursed-lip breathing may help selected patients control expiration and dynamic hyperinflation. Forward-lean sitting, pacing, recovery positions, interval exercise and upper- and lower-limb training are frequently useful. Routine airway clearance offers little benefit when sputum retention is absent (Hillegass, 2022).
For asthma+COPD, physiotherapists should monitor wheeze, chest tightness and symptom variability during exercise. Adequate warm-up, inhaler-technique review and appropriate access to prescribed reliever medication are important. Breathing-control exercises may reduce dysfunctional breathing symptoms but should not replace anti-inflammatory asthma treatment.
In bronchiectasis, airway clearance is a core treatment rather than an optional addition. The ERS recommends that most patients be taught an individualised technique by an appropriately trained professional. Pulmonary rehabilitation is also recommended when exercise capacity is impaired (ERS, 2025). Treatment may include an active cycle of breathing, autogenic drainage, positive expiratory pressure, oscillatory devices, huffing and exercise-assisted clearance. New or worsening haemoptysis, marked desaturation or acute clinical deterioration requires reassessment before continuing the usual programme.

Viva-Ready Summary
- Chronic bronchitis is predominantly an airway and mucus disorder.
- Emphysema is predominantly a disorder of alveolar destruction and hyperinflation.
- Asthma+COPD describes coexisting features of asthma and persistent COPD-related obstruction.
- Bronchiectasis is a CT-confirmed structural airway disorder associated with secretion retention and recurrent infection.
- Spirometry confirms obstruction but cannot always establish the phenotype.
- DLCO is commonly reduced in emphysema and relatively preserved in airway-predominant chronic bronchitis.
- Airway clearance is selective in COPD but central to bronchiectasis management.
- Exercise-based pulmonary rehabilitation remains important across symptomatic chronic respiratory disease.
One-line recall point:
Think mucus in chronic bronchitis, hyperinflation in emphysema, variability in asthma+COPD and recurrent infected sputum with dilated bronchi in bronchiectasis.
References
American Thoracic Society. (2023). Pulmonary rehabilitation for adults with chronic respiratory disease: An official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine, 208(4), e7–e26. https://doi.org/10.1164/rccm.202306-1066ST
European Respiratory Society. (2025). European Respiratory Society clinical practice guideline for the management of adult bronchiectasis. European Respiratory Journal, 66(6), 2501126. https://doi.org/10.1183/13993003.01126-2025
Global Initiative for Asthma. (2025). Global strategy for asthma management and prevention.
Global Initiative for Chronic Obstructive Lung Disease. (2026). Global strategy for prevention, diagnosis and management of chronic obstructive pulmonary disease: 2026 report.
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Main, E., & Denehy, L. (Eds.). (2016). Cardiorespiratory physiotherapy: Adults and paediatrics (5th ed.). Elsevier.
Stanojevic, S., Kaminsky, D. A., Miller, M. R., Thompson, B., Aliverti, A., Barjaktarevic, I., Cooper, B. G., Culver, B., Derom, E., Hall, G. L., Hallstrand, T. S., Leuppi, J. D., MacIntyre, N., McCormack, M., Rosenfeld, M., Swenson, E. R., & Graham, B. L. (2022). ERS/ATS technical standard on interpretive strategies for routine lung function tests. European Respiratory Journal, 60(1), 2101499. https://doi.org/10.1183/13993003.01499-2021