Foundations of Neurological Rehabilitation: A Study Guide
Learn the foundations of neurological rehabilitation, including Bobath/NDT, motor relearning, task-specific training, CIMT, major neurological conditions and essential assessment scales.
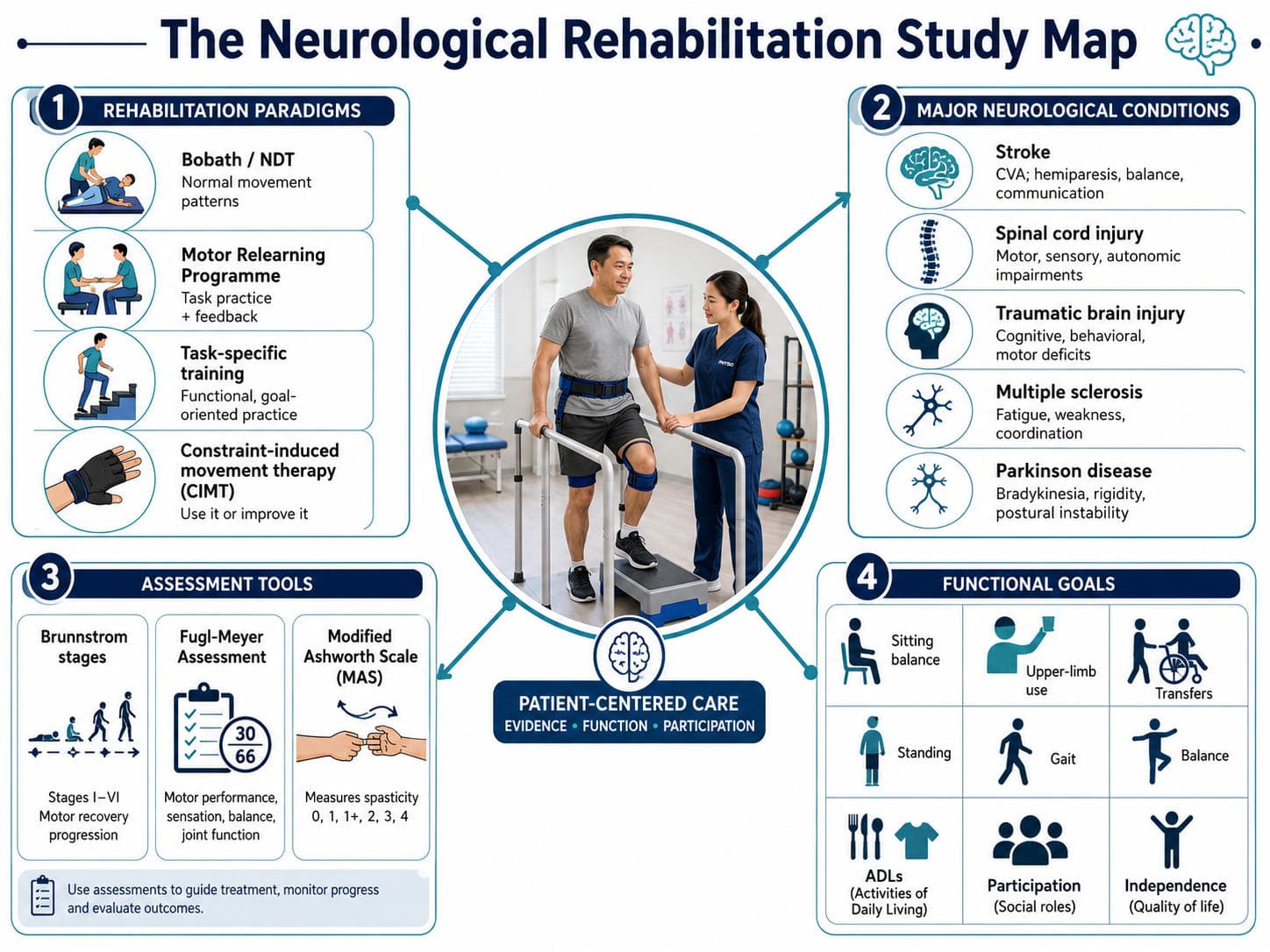
Neurological rehabilitation is a coordinated, patient-centred process that aims to optimise movement, independence, participation and quality of life after injury or disease of the nervous system. It does not simply attempt to “normalise tone". Modern neurorehabilitation combines movement analysis, neuroplasticity, motor learning, exercise prescription, prevention of secondary complications and repeated practice of meaningful activities.
The International Classification of Functioning, Disability and Health provides a useful overall framework. A patient may have an impairment such as weakness or spasticity, an activity limitation such as difficulty walking, and a participation restriction such as inability to return to work. Environmental factors, caregiver support, cognition, motivation and personal goals influence every stage of rehabilitation (World Health Organization [WHO], 2001).
For examinations, neurological rehabilitation is easiest to understand through three linked questions:
- Which rehabilitation paradigm explains the treatment approach?
- Which neurological condition and movement problems are present?
- Which assessment tool measures the impairment or recovery?
The Core Principles Behind Neurorehabilitation
Neurological recovery is influenced by spontaneous biological recovery, compensation, learning and experience-dependent neuroplasticity. Practice must therefore be sufficiently repetitive, challenging, specific and meaningful. Feedback may initially be frequent but should gradually reduce as the patient develops independent error detection.
The physiotherapist should assess the complete movement system rather than focusing on one muscle or reflex. Important domains include:
- Motor control, strength, tone and selective movement
- Sensation, perception, vision and vestibular function
- Balance, coordination, transfers and gait
- Cognition, communication, behaviour and fatigue
- Cardiovascular fitness and exercise tolerance
- Activity performance, participation and patient goals
Modern treatment rarely follows one named approach exclusively. Components from different paradigms may be used, but intervention should remain measurable, goal-directed and supported by current evidence.
Major Neurological Rehabilitation Paradigms

Bobath/NDT in contemporary practice
Bobath remains important in university examinations because it shaped neurological physiotherapy education and emphasised postural control, sensory input and movement quality. However, systematic reviews have not shown Bobath to be superior to other approaches. Task-specific training may produce better upper- and lower-limb activity outcomes after stroke (Dorsch et al., 2023; Scrivener et al., 2020).
Therefore, a balanced viva answer is:
Bobath may contribute movement analysis, positioning and guided practice, but it should not replace adequate strength training, repetition or functional task practice.
Motor relearning and task-specific training
The Motor Relearning Programme treats movement as a skill that can be reacquired. The therapist identifies the functional task, observes performance, determines the missing components, arranges practice and encourages transfer into daily life (Carr & Shepherd, 2010).
Task-specific training extends this principle. Practice should be meaningful, sufficiently intensive and varied enough to prepare the patient for real environments. For example, gait rehabilitation should include starting, stopping, turning, changing speed, avoiding obstacles and walking while carrying objects—not only isolated lower-limb exercises.
Constraint-induced movement therapy
Traditional CIMT combines intensive graded practice, restriction of the less-affected limb and behavioural methods that promote real-world use. Modified protocols use shorter practice periods and are more feasible clinically. CIMT is not suitable for every patient; selection depends on voluntary movement, safety, cognition, pain, fatigue and ability to participate in intensive practice (National Clinical Guideline for Stroke, 2023).
Major Conditions to Study

The same intervention should not be applied identically across these conditions. Stroke and TBI involve acquired brain injury and recovery after a defined event, whereas MS and Parkinson's disease are usually progressive. SCI management is strongly influenced by neurological level, completeness, respiratory involvement and autonomic safety. Current guidance supports active exercise and functional training across these populations, adapted to disease-specific risks and goals (WHO, 2023).
4. Assessment Frameworks: Brunnstrom, Fugl-Meyer and MAS
Brunnstrom stages of motor recovery
The Brunnstrom framework describes the appearance and later reduction of post-stroke limb synergies. It is commonly taught as six stages, although some descriptions add a seventh stage representing near-normal function.
- Stage 1 — Flaccidity
No voluntary movement is present, and the affected muscles are flaccid. - Stage 2 — Beginning spasticity
Basic limb synergies begin to appear, and minimal voluntary movement may be present. - Stage 3 — Marked spasticity
Voluntary control of the basic movement synergies develops, and spasticity reaches its maximum. - Stage 4 — Declining spasticity
Spasticity begins to decrease, and some voluntary movements outside the basic synergies become possible. - Stage 5 — Relative independence from synergies
More complex voluntary movement combinations are performed, with further reduction in the influence of basic synergies. - Stage 6 — Near-normal coordination
Individual joint movements and coordinated movement patterns become possible, and spasticity is minimal or absent.
Brunnstrom staging is clinically quick and useful for describing the pattern of motor return. However, it is an ordinal classification rather than a detailed quantitative outcome measure. Different limbs may also be at different stages.
Fugl-Meyer Assessment
The Fugl-Meyer Assessment is a stroke-specific, performance-based measure of sensorimotor impairment. Its motor items are organised around reflex activity, synergy patterns, movement outside synergy and coordination. Items are usually scored from 0 to 2, where 0 indicates inability, 1 partial performance and 2 complete performance.
The upper-extremity motor score has a maximum of 66, while the lower-extremity motor score has a maximum of 34. Additional sections assess sensation, balance, joint range of motion and joint pain. It is more detailed and responsive than Brunnstrom staging and is widely used in stroke research and clinical rehabilitation (Fugl-Meyer et al., 1975; University of Gothenburg, 2026).
Modified Ashworth Scale
The Modified Ashworth Scale grades resistance encountered during passive movement:
Modified Ashworth Scale — Exact Wording
- 0 — No increase in muscle tone.
- 1 — Slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end of the range of motion when the affected part(s) is moved in flexion or extension.
- 1+ — Slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM.
- 2 — More marked increase in muscle tone through most of the ROM, but affected part(s) easily moved.
- 3 — Considerable increase in muscle tone, passive movement difficult.
- 4 — Affected part(s) rigid in flexion or extension.
A critical viva point is that the MAS does not measure spasticity in isolation. Resistance may also be influenced by contracture, non-neural stiffness, pain, positioning and movement speed. It should therefore be interpreted with range of motion, functional observation and, where necessary, a velocity-dependent measure such as the Modified Tardieu Scale (Bohannon & Smith, 1987; Vidmar et al., 2023).
5. A Practical Clinical-Reasoning Sequence
A reliable neurological assessment can be organised into the following sequence:
Medical stability and precautions → cognition and communication → sensation and perception → tone and selective motor control → functional movement → gait and balance → participation goals
The therapist then converts findings into a prioritised problem list. For example:
Reduced selective ankle dorsiflexion, inadequate weight transfer and fear of falling are limiting safe community walking.
Treatment should directly address this functional problem through strengthening, task-specific stepping, balance training, environmental practice and appropriate assistive-device prescription. Reassessment should use the same standardised measures to determine whether improvement reflects true change rather than subjective observation.

6. Recommended Reading Order
For efficient exam preparation, study neurological rehabilitation in this order:
- Motor control and motor learning: Motor Control: Translating Research into Clinical Practice by Shumway-Cook and colleagues.
- Comprehensive neurological physiotherapy: Umphred’s Neurological Rehabilitation by Lazaro.
- Task-oriented rehabilitation: Neurological Rehabilitation: Optimizing Motor Performance by Carr and Shepherd.
- Condition-specific guidance: Stroke rehabilitation guidelines, SCI physiotherapy guidelines, INCOG guidance for TBI, NICE guidance for MS and the APTA Parkinson's disease guideline.
- Outcome measures: Learn the purpose, scoring, interpretation and limitations of Brunnstrom staging, Fugl-Meyer Assessment and the Modified Ashworth Scale.
Do not memorise techniques without understanding the patient problem they are intended to solve.
7. Viva-Ready Summary
- Neurological rehabilitation aims to improve impairment, activity and participation.
- Bobath/NDT emphasises movement analysis and postural control but is not superior to task-specific rehabilitation.
- Motor relearning uses task analysis, practice, feedback and transfer.
- Task-specific training is the central modern approach to functional recovery.
- CIMT addresses learned non-use in appropriately selected patients after stroke.
- Stroke, SCI, TBI, MS and Parkinson's disease require different precautions and treatment priorities.
- Brunnstrom describes recovery stages, Fugl-Meyer quantifies post-stroke impairment and MAS grades resistance to passive movement.
One-line recall point: Neurological rehabilitation combines condition-specific assessment with repetitive, meaningful and measurable task practice to improve real-life function.
References
Bohannon, R. W., & Smith, M. B. (1987). Interrater reliability of a modified Ashworth scale of muscle spasticity. Physical Therapy, 67(2), 206–207. https://doi.org/10.1093/ptj/67.2.206
Brunnstrom, S. (1970). Movement therapy in hemiplegia: A neurophysiological approach. Harper & Row.
Carr, J. H., & Shepherd, R. B. (2010). Neurological rehabilitation: Optimizing motor performance (2nd ed.). Elsevier.
Dorsch, S., Carling, C., Cao, Z., Fanayan, E., Graham, P. L., McCluskey, A., Schurr, K., Scrivener, K., & Tyson, S. (2023). Bobath therapy is inferior to task-specific training and not superior to other interventions in improving arm activity and arm strength outcomes after stroke: A systematic review. Journal of Physiotherapy, 69(1), 15–22. https://doi.org/10.1016/j.jphys.2022.11.008
Fugl-Meyer, A. R., Jääskö, L., Leyman, I., Olsson, S., & Steglind, S. (1975). The post-stroke hemiplegic patient: A method for evaluation of physical performance. Scandinavian Journal of Rehabilitation Medicine, 7(1), 13–31.
Harb A, Margetis K, Kishner S. Modified Ashworth Scale. [Updated 2025 Apr 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554572/
Lazaro, R. T. (Ed.). (2025). Umphred’s neurological rehabilitation (8th ed.). Elsevier.
National Clinical Guideline for Stroke. (2023). National clinical guideline for stroke for the United Kingdom and Ireland.
National Institute for Health and Care Excellence. (2022). Multiple sclerosis in adults: Management (NICE Guideline NG220; updated 2026).
Scrivener, K., Dorsch, S., McCluskey, A., Schurr, K., Graham, P. L., Cao, Z., Shepherd, R., & Tyson, S. (2020). Bobath therapy is inferior to task-specific training and not superior to other interventions in improving lower-limb activities after stroke: A systematic review. Journal of Physiotherapy, 66(4), 225–235.
University of Gothenburg. (2026). Fugl-Meyer Assessment.
Vidmar, T., Goljar Kregar, N., & Puh, U. (2023). Reliability of the Modified Ashworth Scale after stroke for 13 muscle groups. Archives of Physical Medicine and Rehabilitation, 104(10), 1606–1611. https://doi.org/10.1016/j.apmr.2023.04.008
World Health Organization. (2001). International classification of functioning, disability and health: ICF.
World Health Organization. (2023). Package of interventions for rehabilitation: Module 3—Neurological conditions.