AECOPD in Hospital: The Physiotherapy Protocol from Admission to Discharge
Learn a step-by-step in-hospital physiotherapy protocol for AECOPD, including assessment, NIV, positioning, airway clearance, mobilisation safety and discharge criteria.
An acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is an acute worsening of dyspnoea and/or cough and sputum occurring over a few days, usually up to 14 days, often caused by infection, pollution or another airway insult and requiring additional treatment. During admission, the physiotherapist must balance two priorities: preventing the complications of inactivity while avoiding excessive respiratory demand in an unstable patient.
The physiotherapy protocol can be remembered as:
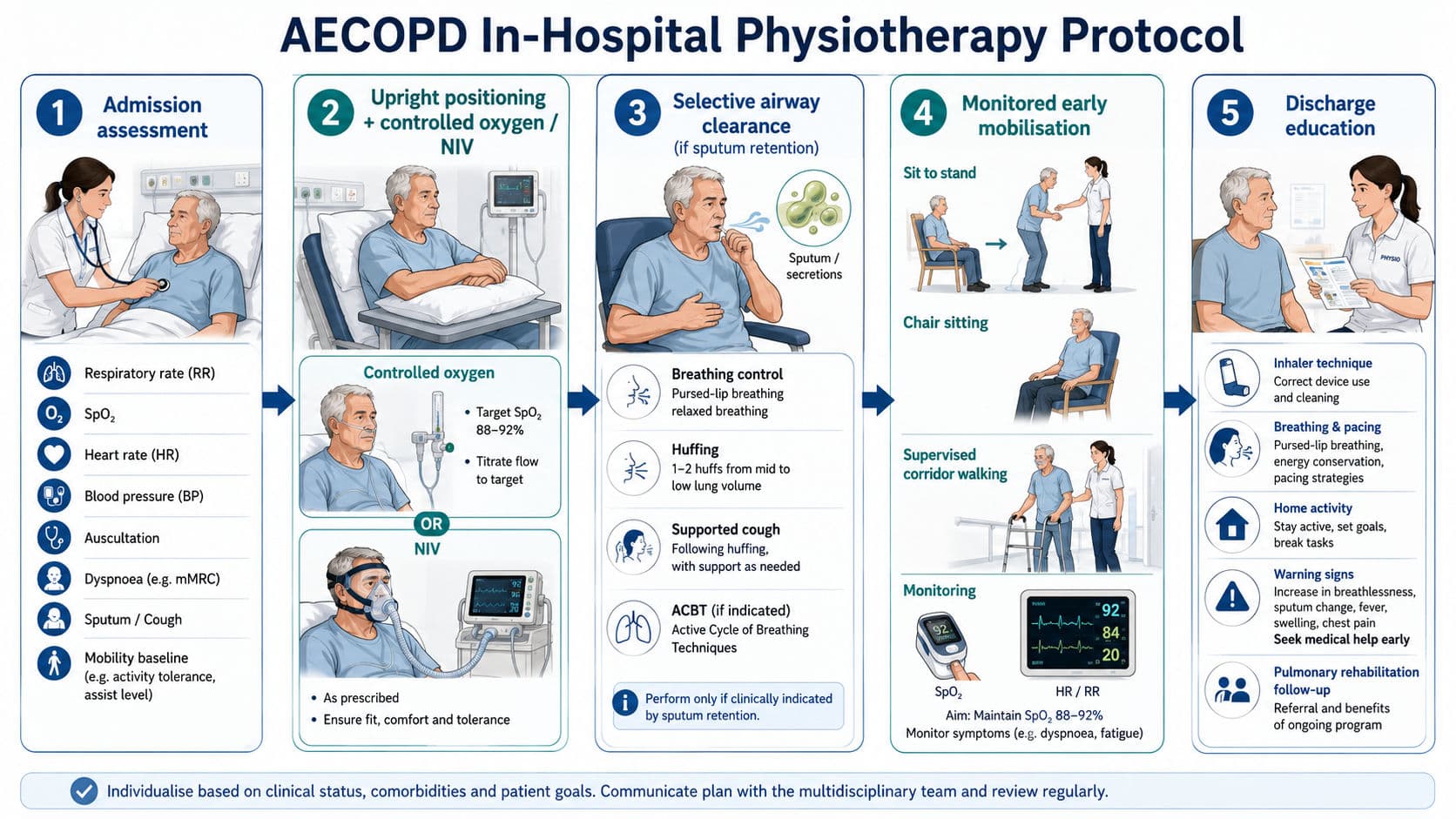
ASSESS → SUPPORT → CLEAR → MOVE → DISCHARGE
Physiotherapy is not automatically synonymous with chest percussion or walking. The correct intervention depends on respiratory stability, sputum retention, ventilatory support and the patient’s previous functional status.
1. ASSESS: Day-of-Admission Physiotherapy Assessment
The initial assessment establishes whether the patient needs immediate respiratory intervention, secretion clearance, mobilisation or escalation to the medical team.
Begin by reviewing the diagnosis, baseline COPD severity, previous exacerbations, home oxygen or non-invasive ventilation use, usual mobility, smoking history and associated conditions such as bronchiectasis, heart failure or pneumonia. Compare current function with the patient’s pre-exacerbation baseline.
The bedside assessment should include:
- Respiratory rate, breathing pattern and accessory-muscle activity
- SpO₂, oxygen-delivery device and prescribed saturation range
- Heart rate, blood pressure, temperature and level of consciousness
- Dyspnoea at rest, ability to speak and modified Borg score
- Chest expansion, auscultation and presence of wheeze or crackles
- Cough strength, sputum volume, colour, viscosity and ease of expectoration
- Bed mobility, sitting balance, transfers and previous walking ability
- Arterial blood gas findings, particularly pH, PaCO₂ and PaO₂
- Chest radiograph findings and possible complications
Pulse oximetry should be recorded with the other vital signs. Arterial blood gases are particularly important when SpO₂ is below 92%, oxygen requirements are increasing, hypercapnia is suspected or the patient has severe airflow limitation. Respiratory acidosis indicates acute ventilatory failure and should prompt consideration of assisted ventilation rather than routine exercise progression (Lung Foundation Australia & Thoracic Society of Australia and New Zealand, 2025).
Clinical pearl: Spirometry is generally not a physiotherapy priority during severe respiratory distress. Previous stable spirometry is more useful than a poorly performed acute test.
2. SUPPORT: Positioning, Oxygen and the Role of NIV
Place the patient in an upright, well-supported position. High sitting or forward-lean sitting with the forearms supported on a table or pillows may reduce breathlessness by stabilising the shoulder girdle and improving accessory-muscle efficiency. Prolonged supine positioning should be avoided where possible.
Oxygen is a treatment for hypoxaemia, not simply for breathlessness. In most patients admitted with AECOPD, controlled oxygen should be titrated to maintain SpO₂ between 88% and 92% until blood gases and an individualised target are available. Uncontrolled high-concentration oxygen may worsen hypercapnia in susceptible patients (National Institute for Health and Care Excellence, 2023).
Non-invasive ventilation, usually bilevel NIV, is indicated when an exacerbation produces acute or acute-on-chronic hypercapnic respiratory failure with respiratory acidosis, generally pH ≤ 7.35 with an elevated PaCO₂, despite appropriate medical management. NIV reduces respiratory-muscle load, improves alveolar ventilation and lowers the need for intubation and mortality (Rochwerg et al., 2017). The 2026 American Thoracic Society guideline continues to strongly recommend NIV for acute hypercapnic respiratory failure; high-flow nasal oxygen is not a routine replacement for NIV in moderate-to-severe hypercapnic acidosis (Goel et al., 2026).

The physiotherapist’s role around NIV may include:
- Optimising upright positioning and mask tolerance
- Coaching relaxed breathing and reducing patient–ventilator fighting
- Observing mask leak, synchrony, respiratory rate and accessory-muscle use
- Coordinating airway clearance, meals and mobilisation around NIV breaks
- Monitoring for worsening acidosis, drowsiness or escalating respiratory distress
- Escalating suspected NIV failure immediately
NIV settings and oxygen changes must follow local scope-of-practice rules and the responsible respiratory or critical-care team.
3. CLEAR: Secretion Clearance During an Exacerbation
Airway-clearance treatment is not required routinely in every AECOPD admission. It is most appropriate when there is sputum retention, an ineffective cough, audible secretions, mucus plugging, lobar collapse or coexisting bronchiectasis.
Treatment should be individualised and usually performed after prescribed bronchodilator therapy. Suitable options include the active cycle of breathing technique, breathing control, thoracic-expansion breaths, forced expiratory technique or huffing, supported coughing and positive expiratory pressure therapy. Oscillating PEP may be considered in patients who regularly produce sputum and can use the device safely.
Short, symptom-limited sessions are usually better tolerated than prolonged aggressive treatment. The patient should be allowed recovery breaths between huffs or coughs to limit dynamic hyperinflation. Routine vigorous percussion is rarely necessary and may increase distress, bronchospasm or oxygen demand in a severely breathless patient.
Current evidence supports selecting airway-clearance techniques according to the sputum-producing phenotype, airflow limitation, dyspnoea, cough effectiveness and patient tolerance rather than applying one technique to every patient (Poncin et al., 2025).
4. MOVE: Early Mobilisation and Progression
Once respiratory and haemodynamic stability is established, prolonged bed rest should be avoided. Hospitalisation rapidly worsens quadriceps strength, balance, confidence and functional independence in COPD.
Progress activity in small steps:

Monitor SpO₂ continuously during the first mobilisation attempt, particularly when oxygen needs have recently changed. Record dyspnoea, respiratory rate, heart rate, symptoms and recovery time. Oxygen should remain at the prescribed flow unless adjustment has been authorised.
Early pulmonary rehabilitation initiated during admission or within four weeks of discharge can improve walking capacity, dyspnoea and health-related quality of life and may reduce readmission risk. However, acute ward activity must remain individually prescribed rather than delivered as high-intensity exercise training (Lu et al., 2023).
5. When NOT to Mobilise: The Red-Light Screen
The oxygen target and the mobilisation threshold are related but not identical. A patient whose prescribed range is 88–92% may be suitable for activity at 89–90%, provided the value is stable and the patient has adequate clinical reserve.
Do not begin active mobilisation or stop the session when:
- Resting SpO₂ is below 88% despite prescribed oxygen or ventilatory support
- SpO₂ falls below the prescribed range and does not recover promptly with rest
- Saturation decreases by more than approximately 4% with symptoms
- Oxygen or NIV requirements are rapidly increasing
- There is severe respiratory distress, exhaustion or a respiratory rate approaching or exceeding 40 breaths/minute
- The patient develops chest pain, a new arrhythmia, marked hypotension or presyncope
- Consciousness is reduced, agitation is worsening or the patient cannot follow safety instructions
- Blood gases show worsening respiratory acidosis
- There is suspected pneumothorax, pulmonary embolism, acute myocardial ischaemia or another untreated complication

Mobilisation safety reviews commonly identify SpO₂ above 88%, together with cardiovascular and neurological stability, as a minimum respiratory criterion. These values are screening limits rather than substitutes for clinical reasoning; patients close to several safety boundaries require multidisciplinary review before mobilisation (Hodgson et al., 2014).
6. DISCHARGE: Physiotherapy and Functional Criteria
Discharge planning should begin during the first 24–48 hours of admission rather than on the final morning.
The patient is generally ready for discharge when clinically stable, free from parenteral treatment for approximately 24 hours, requiring inhaled bronchodilators less frequently than every four hours and able to maintain the prescribed oxygen target. Supplemental oxygen should usually have been discontinued for 24 hours unless long-term or newly prescribed home oxygen is required.
From a physiotherapy perspective, the patient should be able to:
- Transfer and walk safely at or near the required home level
- Manage essential activities of daily living without severe breathlessness
- Complete stairs when these are unavoidable at home
- Use pacing, forward-lean positioning and breathing-control strategies
- Demonstrate an effective huff or airway-clearance technique when indicated
- Understand when worsening breathlessness or sputum requires medical review
- Use mobility aids and oxygen equipment safely
The discharge plan should include inhaler review, medication understanding, smoking-cessation support, a written exacerbation action plan, follow-up arrangements and referral to pulmonary rehabilitation. COPD discharge bundles containing these elements can reduce hospital readmissions (Lung Foundation Australia & Thoracic Society of Australia and New Zealand, 2025).
Viva-Ready Summary
What is the main physiotherapy aim in AECOPD?
To reduce respiratory distress, assist secretion clearance when indicated, prevent functional decline and restore safe mobility without increasing ventilatory failure.
What is the usual oxygen target?
SpO₂ 88–92%, unless an individual target has been prescribed.
When is NIV indicated?
Acute or acute-on-chronic hypercapnic respiratory failure with respiratory acidosis, generally pH ≤7.35.
Does every patient need chest physiotherapy?
No. Airway clearance is indicated primarily when sputum retention or ineffective clearance is present.
When should mobilisation be withheld?
When SpO₂ remains below 88%, respiratory or haemodynamic instability is present, oxygen requirements are escalating or the patient has worsening acidosis or altered consciousness.
One-Line Recall Point
In AECOPD, assess stability first, support ventilation, clear secretions selectively, mobilise above the safety threshold and discharge only when function and self-management are secure.
References
Downie, P. A. (Ed.). (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Lippincott.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Elsevier.
Global Initiative for Chronic Obstructive Lung Disease. (2026). Global strategy for prevention, diagnosis and management of COPD: 2026 report.
Goel, N. N., Ferreyro, B. L., Pitre, T., Lewis, K., Homer-Bouthiette, C., Angriman, F., et al. (2026). Noninvasive respiratory support for adult patients with acute respiratory failure: An official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine. Advance online publication. https://doi.org/10.1093/ajrccm/aamag302
Hillegass, E. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Hodgson, C. L., Stiller, K., Needham, D. M., Tipping, C. J., Harrold, M., Baldwin, C. E., et al. (2014). Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Critical Care, 18, 658.
Lu, H.-Y., Chen, C.-F., Lee, D. L., Tsai, Y.-J., & Lin, P.-C. (2023). Effects of early pulmonary rehabilitation on hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease: A systematic review and meta-analysis. International Journal of Chronic Obstructive Pulmonary Disease, 18, 881–893. https://doi.org/10.2147/COPD.S397361
Lung Foundation Australia & Thoracic Society of Australia and New Zealand. (2025). The COPD-X plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease (Version 2.78).
National Institute for Health and Care Excellence. (2023). Chronic obstructive pulmonary disease in adults: Emergency oxygen during an exacerbation (Quality statement 6).
Poncin, W., et al. (2025). Airway clearance techniques for people with acute exacerbation of chronic obstructive pulmonary disease: A scoping review. European Respiratory Review, 34(175), 240191.
Rochwerg, B., Brochard, L., Elliott, M. W., Hess, D., Hill, N. S., Nava, S., et al. (2017). Official ERS/ATS clinical practice guidelines: Noninvasive ventilation for acute respiratory failure. European Respiratory Journal, 50(2), 1602426. https://doi.org/10.1183/13993003.02426-2016