Cardiac Rehabilitation Phases I–IV: From Hospital Recovery to Lifelong Heart Health
Understand cardiac rehabilitation phases I–IV, the physiotherapist’s role, key outcome measures, and how phases overlap in Indian practice today.
A cardiac event may be treated within hours, but recovery continues long after the patient leaves the hospital. Cardiac rehabilitation bridges this gap. It is a structured, multidisciplinary process whose purpose is not only to help the patient move again but also to restore function, reduce future cardiovascular risk and build confidence for long-term self-management.
Contemporary guidance describes cardiac rehabilitation as a comprehensive, multidisciplinary form of secondary prevention. Its core components include patient assessment, aerobic and strength training, physical-activity counselling, nutritional support, risk-factor management, psychosocial care and outcome evaluation (Brown et al., 2024). Exercise-based programmes can reduce hospital admissions and recurrent cardiovascular events while improving health-related quality of life in people with coronary heart disease (Dibben et al., 2021).
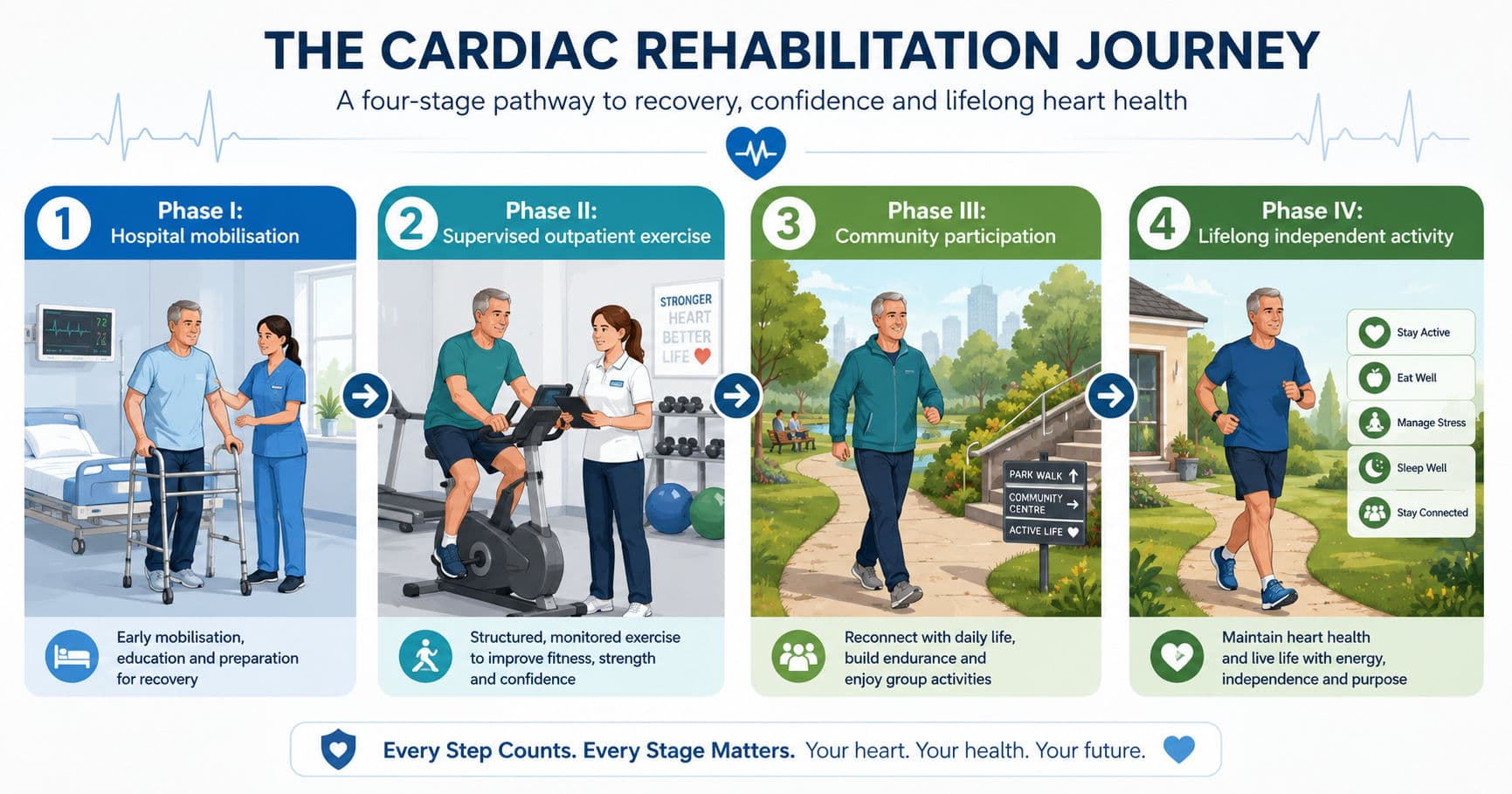
Cardiac rehabilitation is commonly organised into four phases: inpatient rehabilitation, supervised outpatient rehabilitation, community-based rehabilitation and lifelong maintenance.
Cardiac rehabilitation is more than exercise
The overall aim is to help the patient achieve the highest safe level of physical, psychological, social and vocational function. The cardiac rehabilitation team may include a cardiologist, physiotherapist, nurse, dietitian, psychologist and occupational therapist.
The physiotherapist assesses mobility and exercise capacity, initiates safe activity, prescribes and progresses exercise, monitors physiological responses, educates the patient and supports the transition towards independence.
Across all phases, physiotherapy aims to:
- Restore function without provoking cardiovascular instability.
- Prevent deconditioning and secondary complications.
- Recognise symptoms and abnormal physiological responses early.
- Improve exercise capacity through individualised progression.
- Develop safe self-monitoring and long-term exercise behaviour.
The four phases at a glance
| Phase | Usual setting | Primary focus | Physiotherapy contribution |
|---|---|---|---|
| Phase I | Hospital or surgical unit | Safe mobilisation and discharge readiness | Assessment, early mobility, monitoring and education |
| Phase II | Supervised outpatient programme | Structured reconditioning and secondary prevention | Exercise prescription, aerobic and resistance training, monitoring and risk-factor management |
| Phase III | Community, home or hybrid setting | Increasing independence and social participation | Exercise progression, self-monitoring and return to occupational and community roles |
| Phase IV | Independent or community maintenance | Lifelong cardiovascular health | Continued activity, risk-factor control, periodic reassessment and relapse prevention |
The phases naturally overlap. Education for Phase II may begin during admission, a patient attending outpatient sessions may also exercise at home, and maintenance habits begin before formal supervision ends.
Phase I: Safe recovery inside the hospital
Phase I begins when the patient is medically stable after an acute cardiac event or procedure, such as myocardial infarction, percutaneous coronary intervention, coronary artery bypass grafting, valve surgery or hospitalisation for heart failure.
Before mobilisation, the physiotherapist reviews the diagnosis, procedure, haemodynamic status, symptoms, comorbidities, medications, lines and drains, and relevant precautions. Baseline assessment may include heart rate, blood pressure, respiratory rate, oxygen saturation, examining the latest arterial blood gas reports, perceived exertion, transfers and tolerance to simple activity.
Intervention progresses from basic movement towards discharge-level function. It may include positioning, circulatory exercises, bed mobility, sitting out of bed, sit-to-stand practice, short-distance walking and stair assessment when relevant. Breathing exercises, supported coughing or airway clearance techniques are included when clinically indicated rather than routinely prescribed to every patient.
The response to each activity is monitored. New chest discomfort, marked breathlessness, dizziness, pallor, diaphoresis, an abnormal blood pressure response, rhythm disturbance or poor recovery requires reassessment and possible termination of activity.
Before discharge, the patient and family should understand the home walking plan, pacing, warning symptoms, risk-factor modification and the next phase of rehabilitation. Phase I therefore establishes both physical safety and confidence.
Phase II: Supervised outpatient rehabilitation
Phase II is the structured reconditioning stage after discharge. It is commonly delivered over several weeks, although entry and progression depend on medical stability, symptoms, functional capacity, risk stratification and the type of cardiac event or intervention.
The physiotherapist reviews exercise capacity and develops an individualised prescription using the FITT-VP framework:
- Frequency: How often the patient exercises.
- Intensity: How hard the patient works.
- Time: The duration of each session.
- Type: The mode of activity.
- Volume: The total exercise dose.
- Progression: How the programme advances.
Walking and cycle ergometry are commonly used for aerobic conditioning. Resistance training is introduced progressively with appropriate loads, breathing technique and symptom monitoring. Flexibility, balance and functional practice may be added according to the patient’s needs.
Monitoring may include heart rate, blood pressure, oxygen saturation, symptoms, cardiac rhythm when indicated and rating of perceived exertion. Heart-rate targets should not be used alone, especially in patients taking beta-blockers or those with an altered chronotropic response. RPE and the talk test help reflect the intensity that the patient is actually experiencing (Milani et al., 2024).
Phase II also addresses confidence, psychosocial recovery, medication adherence, household activities, return to work and cardiovascular risk factors. The goal is not simply to complete a set number of sessions but to prepare the patient for informed independence.
Phase III: From supervision to community participation
Phase III shifts the emphasis from close clinical supervision to activity in the patient’s own environment. Exercise may take place in a community facility, local gym, home setting or hybrid programme combining occasional centre-based review with remotely supported sessions.
The physiotherapist continues to progress endurance, strength and functional participation. Training becomes increasingly linked to goals such as returning to work, travelling, managing household responsibilities and resuming recreation. The patient learns to modify exercise during fatigue, minor illness or changes in medication.
This phase often overlaps with Phase II. A patient may attend one supervised session each week while completing the remaining sessions at home. Professionally supported home-based and centre-based programmes can produce broadly comparable clinical and quality-of-life outcomes in appropriately selected patients (McDonagh et al., 2023).
Phase IV: Lifelong maintenance
Phase IV maintains the behaviours developed during the earlier stages. It includes regular aerobic and resistance exercise, reduced sedentary time, medication adherence, risk-factor control, healthy dietary behaviour and attention to psychological wellbeing.
Direct supervision is usually minimal, but periodic reassessment may be needed after a new symptom, hospital admission, change in medical status or prolonged interruption in activity.
The key outcome is self-efficacy: the patient can plan activity, regulate effort, recognise abnormal symptoms and seek professional help appropriately. Phase IV is therefore not the end of rehabilitation. It is the point at which rehabilitation becomes part of everyday life.
Key outcome measures: 6MWT, METs and RPE
Three measures frequently appear in cardiac-rehabilitation examinations and clinical documentation.
Six-minute walk test
The 6-minute walk test, or 6MWT, records the distance walked in six minutes and provides a practical estimate of submaximal functional exercise capacity. It can establish a baseline, guide functional goals and document change during rehabilitation. Distance should be interpreted alongside symptoms, RPE, heart rate, blood pressure and oxygen saturation. Standardised instructions and testing conditions are essential when comparing repeated results.
Metabolic equivalents
Metabolic equivalents, or METs, express the energy demand of an activity or the capacity achieved during exercise testing. One MET is conventionally approximated as an oxygen uptake of 3.5 mL/kg/min.
MET values help clinicians compare the demands of walking, stair climbing, household tasks and recreational activities with the patient’s functional capacity. However, MET values are estimates and should be interpreted together with symptoms and physiological responses.
Rating of perceived exertion
Rating of perceived exertion, or RPE, records how hard the patient feels they are working. The Borg 6–20 scale and CR10 scale are commonly used.
RPE is especially useful when medication blunts the heart-rate response, but it complements rather than replaces objective physiological monitoring.

How the phases overlap in Indian practice
The four-phase framework remains useful, but delivery in India is shaped by short hospital stays, travel distance, cost, work and family responsibilities, uneven referral pathways and limited access to dedicated programmes. A national audit identified a major mismatch between cardiac rehabilitation needs and available capacity, alongside financial and referral barriers (Babu et al., 2020).
Some patients therefore move directly from inpatient mobilisation to a home walking plan, with outpatient review when feasible. Others receive hybrid rehabilitation involving initial supervised sessions followed by telephone calls, digital applications, wearable monitoring or periodic centre visits. Recent Indian expert consensus supports hybrid rehabilitation as a practical way to combine clinical supervision with accessible home-based care while emphasising appropriate monitoring and attention to digital literacy (Shah et al., 2026).
The setting may change, but the essential elements must remain: appropriate assessment, individualised exercise prescription, education, risk-factor management, psychosocial support and outcome review. The four phases are therefore best understood as one continuous patient journey—from safe hospital mobilisation to lifelong heart health.
Viva-ready summary
- Cardiac rehabilitation is a comprehensive, multidisciplinary secondary prevention programme—not exercise alone.
- Phase I focuses on safe inpatient mobilisation and discharge preparation.
- Phase II provides supervised outpatient reconditioning, while Phase III develops community and home independence.
- Phase IV supports lifelong exercise, risk-factor control and self-management.
- The 6MWT measures functional exercise capacity; METs describe activity demand or capacity; and RPE reflects perceived effort.
- In Indian practice, the phases frequently overlap through home-based and hybrid delivery.
References
Babu, A. S., Turk-Adawi, K., Supervia, M., Lopez-Jimenez, F., Contractor, A., & Grace, S. L. (2020). Cardiac rehabilitation in India: Results from the International Council of Cardiovascular Prevention and Rehabilitation’s global audit of cardiac rehabilitation. Global Heart, 15(1), Article 28. https://doi.org/10.5334/gh.783
Brown, T. M., Pack, Q. R., Aberegg, E., Brewer, L. C., Ford, Y. R., Forman, D. E., Gathright, E. C., Khadanga, S., Ozemek, C., & Thomas, R. J. (2024). Core components of cardiac rehabilitation programmes: 2024 update: A scientific statement from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation, 150(18), e328–e347. https://doi.org/10.1161/CIR.0000000000001289
Dibben, G., Faulkner, J., Oldridge, N., Rees, K., Thompson, D. R., Zwisler, A.-D., & Taylor, R. S. (2021). Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database of Systematic Reviews, 2021(11), Article CD001800. https://doi.org/10.1002/14651858.CD001800.pub4
McDonagh, S. T. J., Dalal, H., Moore, S., Clark, C. E., Dean, S. G., Jolly, K., Cowie, A., Afzal, J., & Taylor, R. S. (2023). Home-based versus centre-based cardiac rehabilitation. Cochrane Database of Systematic Reviews, 2023(10), Article CD007130. https://doi.org/10.1002/14651858.CD007130.pub5
Milani, J. G. P. O., Milani, M., Verboven, K., Cipriano, G., Jr., & Hansen, D. (2024). Exercise intensity prescription in cardiovascular rehabilitation: Bridging the gap between best evidence and clinical practice. Frontiers in Cardiovascular Medicine, 11, Article 1380639. https://doi.org/10.3389/fcvm.2024.1380639
Pryor, J. A., & Webber, B. A. (Eds.). (1998). Physiotherapy for respiratory and cardiac problems (2nd ed.). Churchill Livingstone.
Shah, J., Navasundi, G. B., Kumar, S., Kumar, S., & Gharat, C. (2026). Indian expert consensus on hybrid cardiac rehabilitation in the management of cardiovascular disease. Cureus, 18(4), Article e107135. https://doi.org/10.7759/cureus.107135


