Oxygen Therapy and Exercise Prescription in Chronic Lung Disease: A Bedside Guide for Physiotherapists
A bedside physiotherapy guide to oxygen devices, FiO₂ ranges, ambulatory oxygen criteria, SpO₂ targets and exercise prescription in chronic lung disease.
Why Oxygen Therapy Matters During Rehabilitation
In chronic lung disease, oxygen therapy is not given simply because a patient feels breathless. It is prescribed to correct hypoxaemia, reduce physiological stress during activity and allow safer participation in rehabilitation. Breathlessness and oxygen desaturation are related but not identical: a patient may be severely dyspnoeic with acceptable SpO₂, while another may desaturate silently during walking. This is why physiotherapists must combine symptoms, pulse oximetry, work of breathing, heart rate response and functional performance before progressing exercise.
Current guidance supports long-term oxygen therapy for selected patients with severe chronic resting hypoxaemia and ambulatory oxygen for patients who demonstrate severe exertional desaturation, especially when oxygen improves walking tolerance or symptoms (Jacobs et al., 2020). Severe exertional hypoxaemia is commonly defined as SpO₂ ≤ 88% during exertion (Jacobs et al., 2020). GOLD continues to emphasise that oxygen should not be used routinely for moderate resting or exercise-induced desaturation in stable COPD but remains important in severe resting hypoxaemia (Global Initiative for Chronic Obstructive Lung Disease [GOLD], 2026).
Common Oxygen Devices and Approximate FiO₂ Ranges
Oxygen devices differ in how precisely they deliver FiO₂. Low-flow devices, such as nasal cannulae, provide variable FiO₂ because the delivered oxygen mixes with room air and depends on respiratory rate, tidal volume and mouth breathing. Fixed-performance devices, such as Venturi masks, are preferred when controlled oxygen delivery is needed, especially in patients at risk of CO₂ retention.

These FiO₂ values are approximate, not absolute. A tachypnoeic patient on nasal cannula may receive a lower effective FiO₂ than expected, while an anxious mouth-breather may not benefit adequately from low-flow nasal oxygen. HFNC allows independent adjustment of flow and FiO₂, but it is usually a monitored-care device rather than a routine ambulatory rehabilitation device (Weekley et al., 2025).
Target Saturation: The Physiotherapy “Safety Zone”
For most stable chronic lung disease patients during rehabilitation, a practical exercise target is to keep SpO₂ at or above 90%, unless the medical team has prescribed a different range. In COPD or any condition with risk of hypercapnic respiratory failure, controlled oxygen is safer, and a target SpO₂ of 88–92% is commonly recommended until blood gases confirm that a higher target is safe (O’Driscoll et al., 2017). The physiotherapist should therefore check the oxygen prescription before exercise rather than increasing oxygen casually.
A useful bedside rule is treat the target range, not the number alone. For example, a COPD patient with a prescribed target of 88–92% who is walking at 91% may be safe, while pushing them to 98% with high-flow oxygen may be inappropriate. Conversely, an ILD patient who falls from 96% at rest to 84% while walking requires exercise modification, oxygen titration and medical review if desaturation is marked or persistent. BTS guidance stresses target-based oxygen rather than liberal oxygen administration, particularly in patients at risk of hypercapnia (O’Driscoll et al., 2017).
Ambulatory Oxygen Criteria: What Physiotherapists Should Look For
Ambulatory oxygen is considered when the patient is not severely hypoxaemic at rest but desaturates during activity. The most practical assessment is a supervised walking test, commonly the 6-minute walk test, shuttle walk test or a ward-based functional walk where SpO₂, dyspnoea and distance are recorded.
A typical ambulatory oxygen assessment includes three questions:
- Does SpO₂ fall to ≤88% during room-air exertion?
- Does supplemental oxygen correct or meaningfully reduce desaturation?
- Does oxygen improve walking distance, dyspnoea, recovery time or functional confidence?
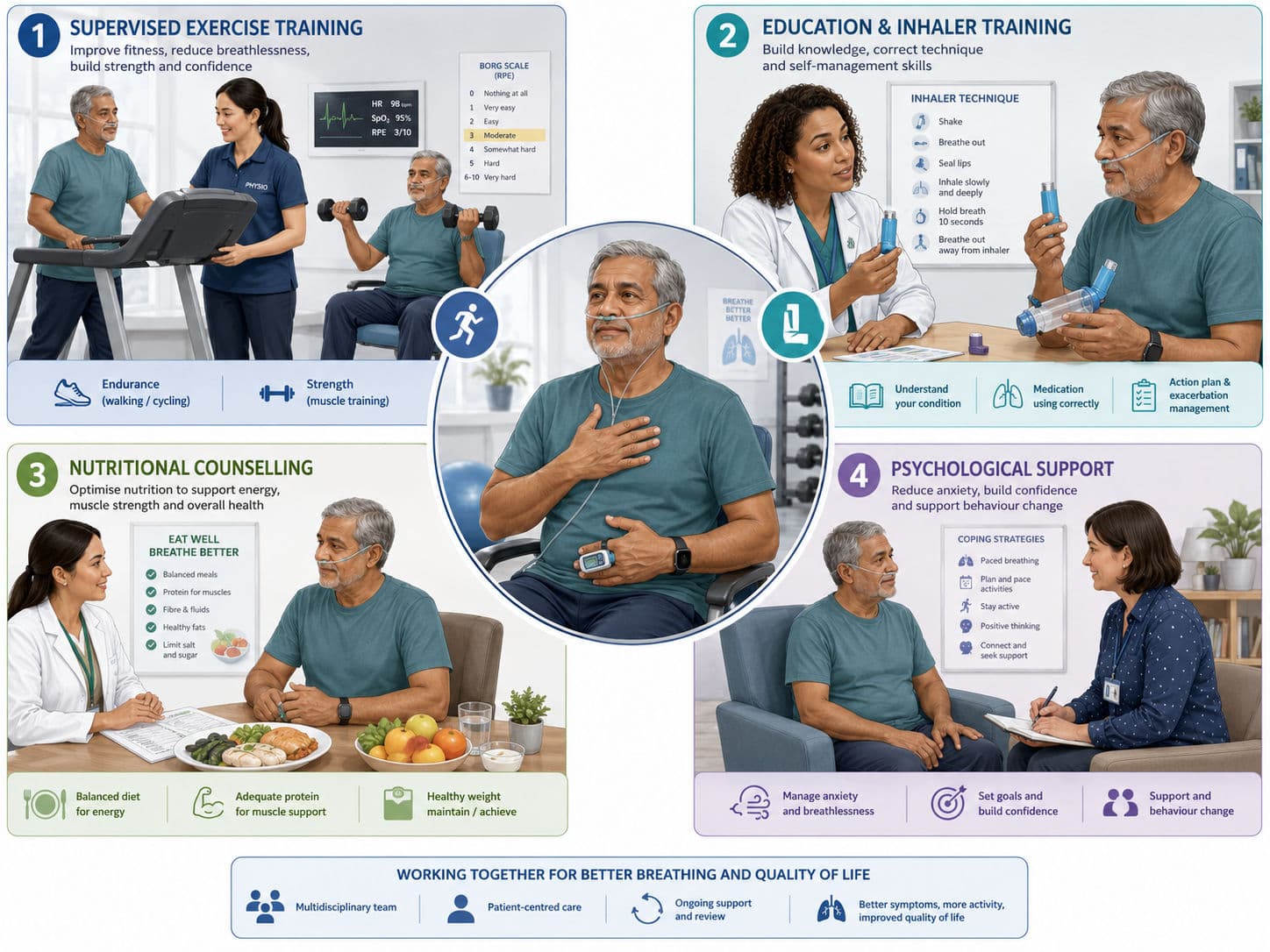
ATS guidance suggests ambulatory oxygen for adults with COPD or ILD who have severe exertional room-air hypoxaemia, although the recommendation is conditional because benefits vary between patients (Jacobs et al., 2020). Oxygen during exercise can acutely improve endurance in some desaturating patients, but it does not replace pulmonary rehabilitation; the core intervention remains progressive exercise training, education and self-management (Rochester et al., 2023).

Exercise Prescription With Oxygen: Practical Bedside Progression
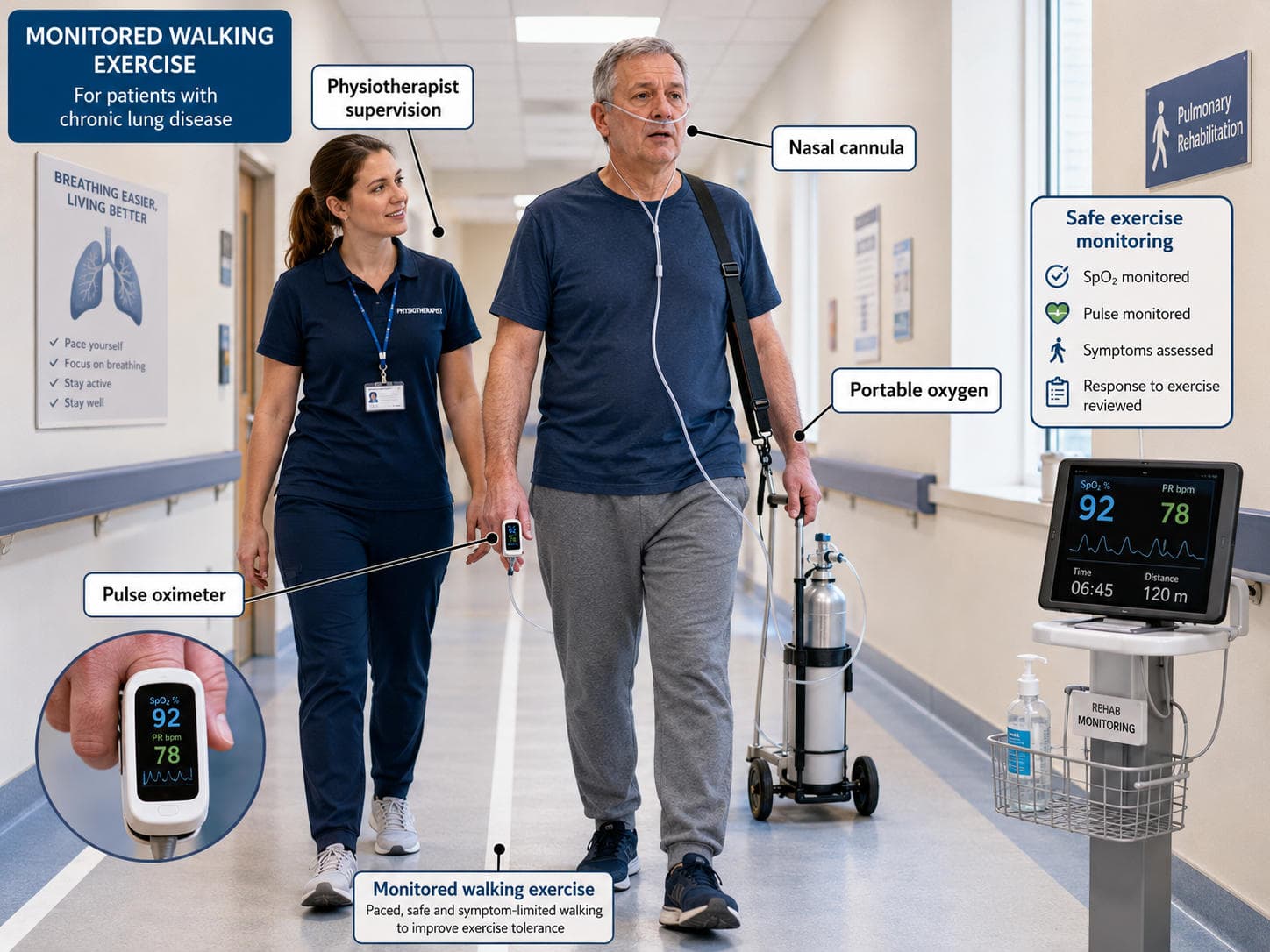
Exercise prescription should start with assessment, not with a fixed walking distance. Record resting SpO₂, device and flow rate, heart rate, blood pressure, dyspnoea score, fatigue and baseline mobility. During exercise, monitor SpO₂ continuously or at frequent intervals, especially during the first session or after oxygen changes.
For aerobic training, walking and cycling are commonly prescribed for 20–30 minutes, 3–5 days per week, using continuous or interval formats. Intensity can be guided by 60–80% of peak walking speed, Borg dyspnoea of about 3–5/10, or a “moderate to somewhat hard” effort. In frail or highly symptomatic patients, interval training is often better tolerated: for example, 1–2 minutes of walking followed by rest, repeated several times. Resistance training may be added 2–3 days per week using 1–3 sets of 8–12 repetitions for major muscle groups, while maintaining breathing control and avoiding prolonged breath-holding (Hillegass, 2022; Frownfelter & Dean, 2022).
The physiotherapist should not chase SpO₂ by oxygen alone. First, correct posture, pacing, breathing pattern, device position, tubing length and probe accuracy. Then consider titration if the patient remains below target.
When to Titrate Oxygen Up During Exercise
Oxygen may need to be increased during exercise when SpO₂ falls below the prescribed target and does not recover quickly with pacing, rest or breathing control. In many bedside settings, nasal cannula oxygen is increased gradually, usually by 1 L/min at a time, followed by reassessment of SpO₂, dyspnoea and heart rate. If the patient is on a Venturi mask, titration usually means changing to a higher fixed FiO₂ device according to prescription or local protocol.
Titrate up or stop exercise when there is persistent SpO₂ below target, sudden desaturation, increasing cyanosis, dizziness, chest pain, confusion, a new arrhythmia, disproportionate tachycardia, severe breathlessness, poor recovery or signs of respiratory fatigue. If the patient needs rapidly escalating oxygen, requires a non-rebreather mask to maintain saturation, or cannot recover after stopping exercise, this is no longer routine rehabilitation; it requires escalation to the medical team.

For COPD or suspected CO₂ retainers, increasing oxygen above the prescribed target should be done cautiously and ideally with ABG guidance. Oxygen corrects hypoxaemia, but it does not ventilate the patient or remove CO₂. If drowsiness, headache, bounding pulse, worsening acidosis or reduced respiratory drive appears, the concern is ventilatory failure, not simply “low oxygen".
Viva-Ready Summary
Oxygen therapy in chronic lung disease is a targeted intervention to correct hypoxaemia and support safe activity, not a treatment for breathlessness alone. Nasal cannulae are comfortable but variable; Venturi masks provide controlled FiO₂, non-rebreather masks are for short-term high oxygen needs, and HFNC provides heated humidified high-flow oxygen in selected monitored settings. During exercise, physiotherapists should maintain the prescribed SpO₂ target, commonly ≥90% in many chronic lung disease patients and 88–92% in COPD or hypercapnia risk patients. Ambulatory oxygen is considered when exertional SpO₂ falls to ≤88% and improves with oxygen. Exercise should still be prescribed progressively using endurance, interval and resistance training principles, with oxygen titrated only when clinically indicated.
One-line recall point:
Prescribe exercise from function, titrate oxygen to target SpO₂, and escalate when desaturation persists despite rest, pacing and appropriate oxygen adjustment.
References
Downie, P. A. (Ed.). (1993). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Jaypee Brothers.
Frownfelter, D., & Dean, E. (2022). Cardiovascular and pulmonary physical therapy: Evidence and practice (6th ed.). Elsevier.
Global Initiative for Chronic Obstructive Lung Disease. (2026). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2026 report. GOLD.
Hillegass, E. A. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Jacobs, S. S., Krishnan, J. A., Lederer, D. J., Ghazipura, M., Hossain, T., Tan, A. Y. M., Carlin, B., Drummond, M. B., Ekström, M., Garvey, C., Graney, B., Jackson, B., Kenn, K., Kim, V., Kummer, F., Ryerson, C. J., Schneidman, A., Swigris, J. J., Upson, D., & Wilson, K. C. (2020). Home oxygen therapy for adults with chronic lung disease: An official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine, 202(10), e121–e141. https://doi.org/10.1164/rccm.202009-3608ST
O’Driscoll, B. R., Howard, L. S., Earis, J., Mak, V., & British Thoracic Society Emergency Oxygen Guideline Group. (2017). BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax, 72(Suppl 1), ii1–ii90. https://doi.org/10.1136/thoraxjnl-2016-209729
Rochester, C. L., Alison, J. A., Carlin, B., Jenkins, A. R., Cox, N. S., Bauldoff, G., Bhatt, S. P., Bourbeau, J., Brooks, D., Holland, A. E., Limberg, T. M., Osadnik, C. R., Pitta, F., Singh, S. J., Steiner, M., & Spruit, M. A. (2023). Pulmonary rehabilitation for adults with chronic respiratory disease: An official American Thoracic Society clinical practice guideline. American Journal of Respiratory and Critical Care Medicine, 208(4), e7–e26. https://doi.org/10.1164/rccm.202306-1066ST
Weekley, M. S., Bland, L. E., & Bissell, B. D. (2025). Oxygen administration. In StatPearls. StatPearls Publishing.