ICU Physiotherapy: Scope, Roles and Assessment at the Bedside
A student-friendly ICU physiotherapy guide covering respiratory care, positioning, mobilisation, ventilator-weaning support, assessment, common ICU conditions and contraindications.
Why ICU Physiotherapy Matters
The intensive care unit is not only a place for ventilators, monitors and emergency drugs. It is also where the prevention of weakness, secretion retention, atelectasis, delirium-related immobility and delayed functional recovery must begin. ICU physiotherapy focuses on maintaining cardiorespiratory function, preventing complications of bed rest and helping the patient move safely from critical illness toward recovery.
Traditionally, ICU care was centred on survival. Modern critical care also recognises post-intensive care syndrome, which includes physical weakness, cognitive issues and psychological distress after ICU discharge. Prolonged immobility, mechanical ventilation, inflammation, sedation and multi-organ dysfunction can rapidly reduce muscle strength and functional independence (Schaller et al., 2024). Therefore, ICU physiotherapy is not an “extra” service; it is part of early, goal-directed critical care.
For physiotherapy students, the ICU must be understood through one simple principle: treat only after screening, and progress only according to physiological response.
Scope of ICU Physiotherapy
The scope of ICU physiotherapy is broad but always patient-specific. A physiotherapist may work with an unconscious ventilated patient, an awake patient on non-invasive ventilation, a postoperative cardiac patient, a patient with sepsis, or a tracheostomised patient learning to sit and stand again.
The major ICU physiotherapy roles include:

The ICU Physiotherapy Assessment
A good ICU session begins before touching the patient. The first step is chart review and discussion with the bedside team. The physiotherapist checks diagnosis, reason for ICU admission, ventilatory support, oxygen requirement, haemodynamic status, sedation level, medications, lines, drains, recent imaging, lab values and medical goals for the day.
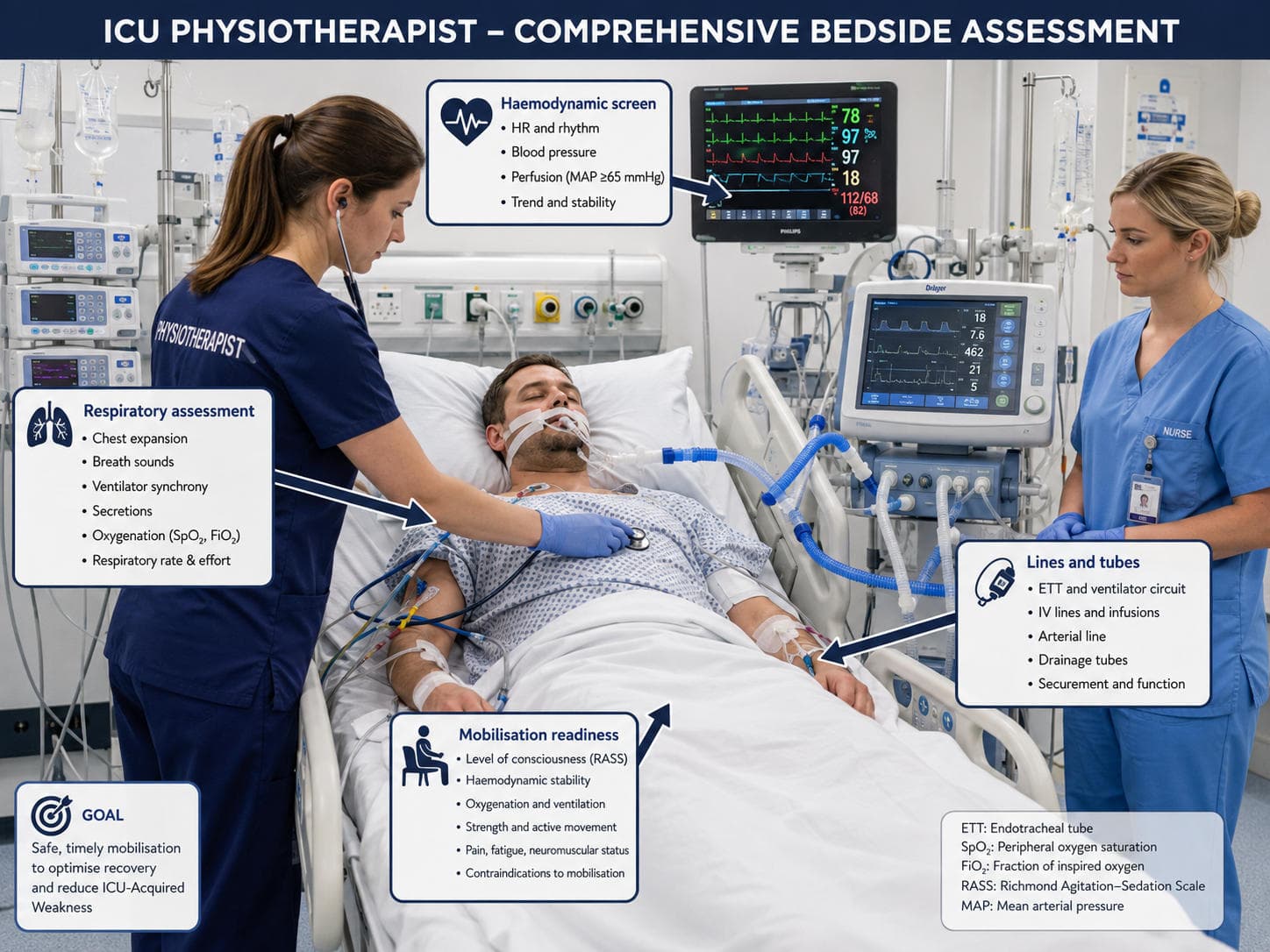
Assessment should include:
1. Respiratory assessment: respiratory rate, breathing pattern, oxygen saturation, oxygen device or ventilator mode, FiO₂, PEEP, auscultation findings, secretion load, cough effectiveness and chest expansion.
2. Cardiovascular assessment: heart rate, rhythm, blood pressure, mean arterial pressure, vasopressor requirement, perfusion, symptoms and response to position change.
3. Neurological assessment: consciousness, command following, agitation, delirium risk, pain, anxiety and ability to participate.
4. Musculoskeletal and functional assessment: range of motion, muscle strength, limb oedema, tone, bed mobility, sitting balance and prior functional level.
5. Safety assessment: endotracheal tube, tracheostomy, arterial line, central line, drains, surgical wounds, fractures, open abdomen, intracranial pressure concerns and infection precautions.

The key question is not “Can I do physiotherapy?” but “What level of physiotherapy is safe today?” For one patient, the correct intervention may be positioning and passive movements. For another, it may be standing or walking with a ventilator.
Core Roles: Respiratory Care, Positioning, Mobilisation and Weaning Support
Respiratory physiotherapy is most useful when there is a clear problem: retained secretions, atelectasis, weak cough, reduced lung volume or difficulty clearing sputum. Techniques may include positioning, ventilator-supported hyperinflation where appropriate, manual techniques, suction assistance, thoracic expansion exercises, huffing or cough facilitation in awake patients. Routine chest physiotherapy for every ventilated patient is not the goal; targeted treatment based on assessment is better clinical practice (Gosselink et al., 2008; van der Lee et al., 2024).
Positioning is one of the simplest but most powerful ICU interventions. Upright positioning can improve diaphragmatic mechanics, reduce work of breathing and prepare the patient for mobilisation. Side-lying may be used for secretion drainage or ventilation distribution, while prone positioning is medically led in selected ARDS patients. The physiotherapist’s role is to understand the respiratory aim, protect lines and pressure areas, and reassess response.
Early mobilisation includes a graded progression: passive range of motion, active-assisted movement, active exercises, bed mobility, sitting over the edge of the bed, sit-outs, standing, marching and walking. Current guidance supports enhanced mobilisation and rehabilitation over usual care when patients are appropriately screened (Lewis et al., 2025). However, early does not mean aggressive. High-quality ICU mobilisation is progressive, monitored and stopped when the patient becomes unstable.

In ventilator weaning, the physiotherapist supports but does not independently “wean the ventilator". Useful contributions include secretion clearance, positioning, improving alertness through mobility, inspiratory muscle training in selected patients, cough assessment, endurance training and functional preparation for extubation or tracheostomy weaning. Physiotherapy interventions such as early mobilisation and inspiratory muscle training have been studied as supportive strategies during mechanical ventilation liberation, although the exact dosage must be individualised (Lippi et al., 2022).
The Multidisciplinary Team in ICU
ICU physiotherapy is never isolated. The physiotherapist works with intensivists; nurses; respiratory therapists, where available; dietitians; pharmacists; occupational therapists; speech and swallow therapists; psychologists; and family caregivers. The nurse is especially central because safe mobilisation depends on line management, sedation status, monitoring and timing with daily care.
A useful ICU communication framework is the following:
- What is the medical goal today?
- Is the patient stable enough for activity?
- What lines, tubes or precautions matter?
- What is the highest safe mobility level today?
- What response would make us stop?
This team-based approach prevents both extremes: unnecessary bed rest and unsafe over-treatment.
Common Conditions Encountered in ICU
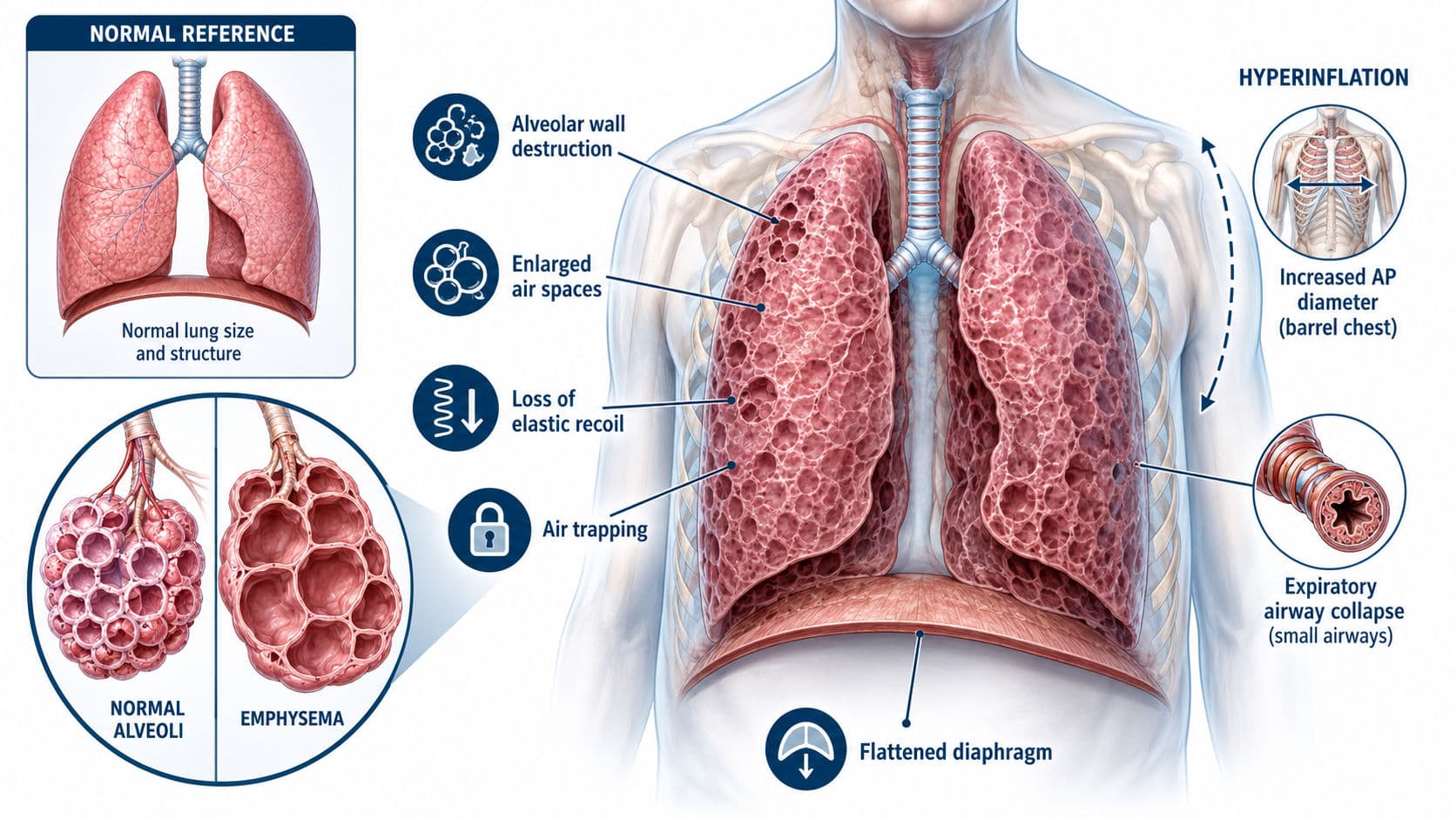
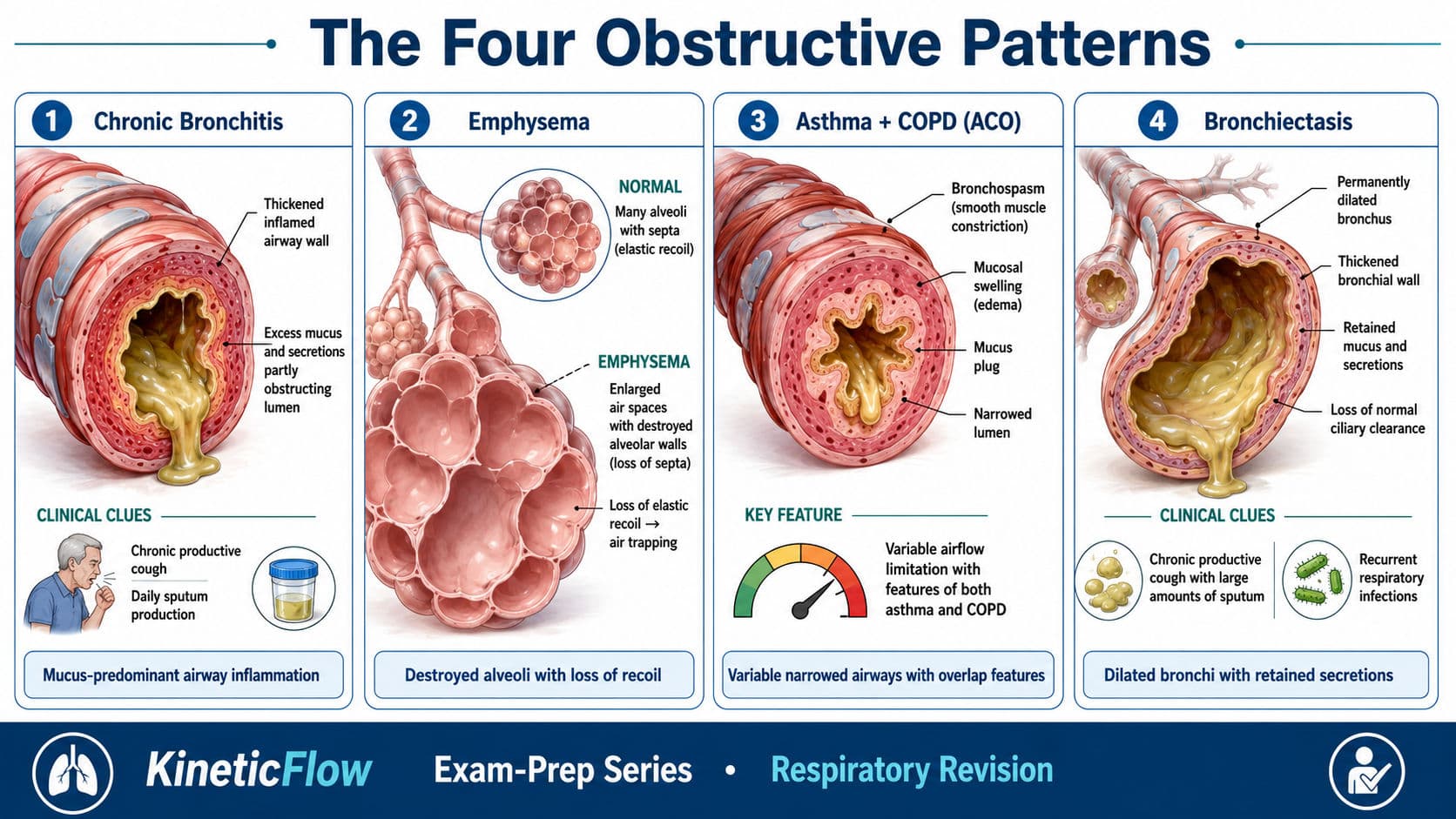
ICU physiotherapists commonly manage patients with acute respiratory failure, pneumonia, ARDS, COPD exacerbation, post-operative cardiac or abdominal surgery, sepsis, trauma, neurological conditions, prolonged mechanical ventilation and tracheostomy. Each condition changes the physiotherapy priority.
For example, a patient with pneumonia may need positioning, secretion management and gradual mobilisation. A post-CABG patient may need breathing exercises, supported coughing, sternal precautions and early walking. A patient with sepsis may initially tolerate only passive movement and positioning because of haemodynamic instability. A tracheostomised patient may require airway clearance, humidification awareness, cuff status discussion and progressive mobility.
The common thread is clinical reasoning. The diagnosis guides the likely problems, but the bedside assessment decides the treatment.
Contraindications and Red Flags in ICU Physiotherapy
Contraindications in ICU are often relative rather than absolute. A patient may be unsuitable for walking but still suitable for positioning or passive movement. The safest approach is to classify findings as green, yellow or red.

During any ICU intervention, stop or downgrade if there is persistent desaturation, sudden hypotension or hypertension, new arrhythmia, marked tachypnoea, reduced consciousness, severe distress, line displacement or clinician concern. A safe ICU physiotherapist is not the one who mobilises everyone; it is the one who knows when to progress, modify, pause or escalate.
Viva-Ready Summary
ICU physiotherapy includes respiratory care, positioning, early mobilisation, functional rehabilitation and ventilator-weaning support. The physiotherapist assesses respiratory status, haemodynamics, consciousness, strength, function, lines and medical precautions before deciding the safest treatment level. ICU physiotherapy is multidisciplinary and should be progressive, monitored and individualised. It is especially important for preventing secretion retention, atelectasis, ICU-acquired weakness and delayed recovery.
One-line recall point: ICU physiotherapy is safe, screened bedside rehabilitation that protects the lungs, preserves movement and supports recovery from critical illness.
References
Anekwe, D. E., Biswas, S., Bussières, A., & Spahija, J. (2020). Early rehabilitation reduces the likelihood of developing intensive care unit-acquired weakness: A systematic review and meta-analysis. Physiotherapy, 107, 1–10.
Downie, P. A., Innocenti, D. M., & Jackson, S. E. (1987). Cash’s textbook of chest, heart and vascular disorders for physiotherapists (4th ed.). Mosby.
Frownfelter, D., Dean, E., Stout, M., Kruger, R., & Anthony, J. (2022). Cardiovascular and pulmonary physical therapy: Evidence to practice (6th ed.). Elsevier.
Gosselink, R., Bott, J., Johnson, M., Dean, E., Nava, S., Norrenberg, M., Schönhofer, B., Stiller, K., van de Leur, H., & Vincent, J. L. (2008). Physiotherapy for adult patients with critical illness: Recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force. Intensive Care Medicine, 34, 1188–1199.
Hillegass, E. A. (2022). Essentials of cardiopulmonary physical therapy (5th ed.). Elsevier.
Lewis, K., Balas, M. C., Stollings, J. L., et al. (2025). A focused update to the clinical practice guidelines for the prevention and management of pain, anxiety, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Critical Care Medicine, 53(3), e711–e727.
Lippi, L., de Sire, A., D’Abrosca, F., Polla, B., Marotta, N., Castello, L. M., Ammendolia, A., Molinari, C., & Invernizzi, M. (2022). Efficacy of physiotherapy interventions on weaning in mechanically ventilated critically ill patients: A systematic review and meta-analysis. Frontiers in Medicine, 9, 889218.
Schaller, S. J., Scheffenbichler, F. T., Bein, T., Blobner, M., et al. (2024). Guideline on positioning and early mobilisation in the critically ill by an expert panel. Intensive Care Medicine. https://doi.org/10.1007/s00134-024-07532-2
van der Lee, L., Patman, S., & Hill, A. M. (2024). Development of a clinical practice guideline for physiotherapy management of adults invasively ventilated with community-acquired pneumonia. Physiotherapy. https://doi.org/10.1016/j.physio.2023.12.003